Prediabetes
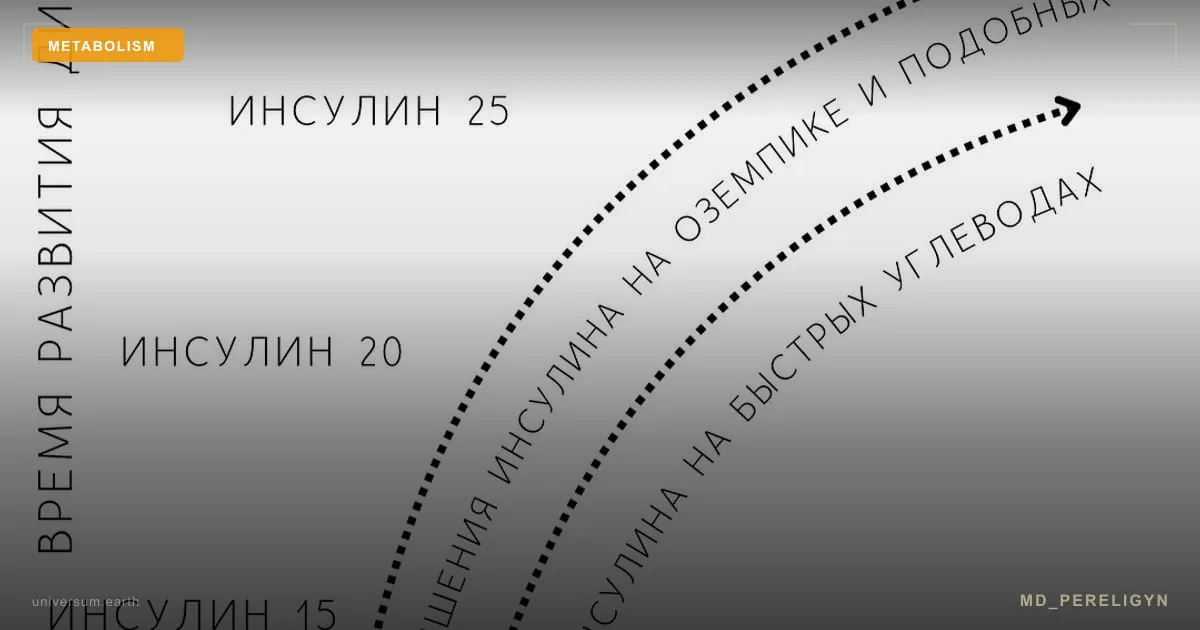
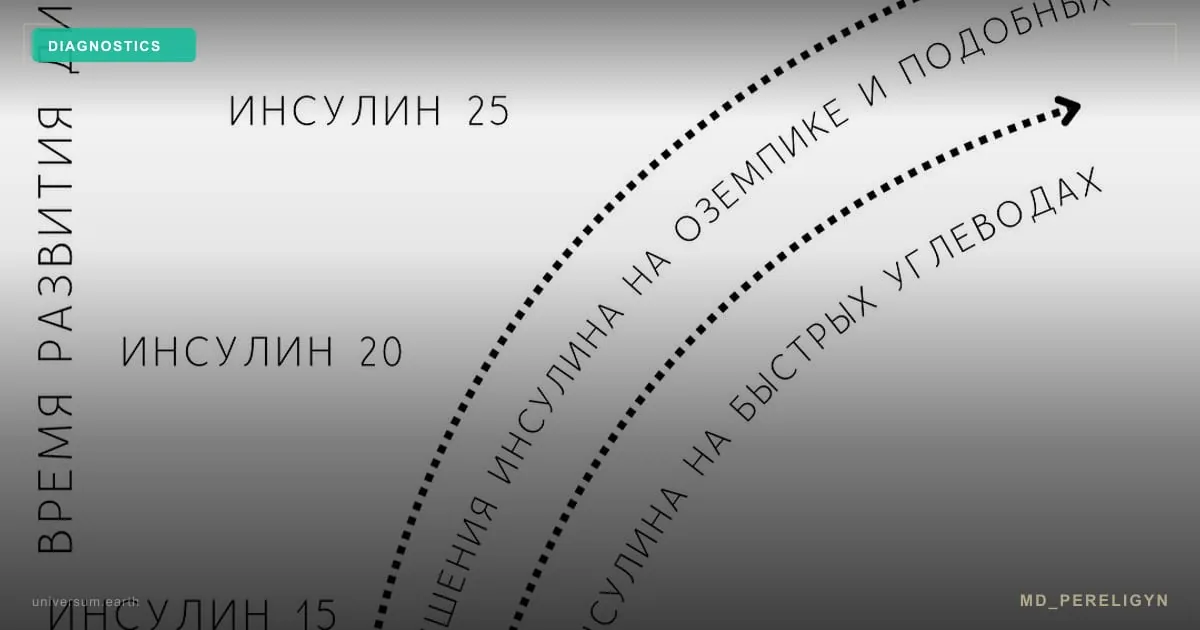
Intermediate dysglycaemia defined by HbA1c 5.7–6.4%, fasting glucose 5.6–6.9 mmol/L, or 2-hour OGTT glucose 7.8–11.0 mmol/L. Prevalence exceeds 35% of adults. Hallmarks include insulin resistance and postprandial hyperinsulinaemia preceding overt fasting hyperglycaemia by years, often with normal routine lab panels.