The Most Important Test Nobody Orders
In 15 years of clinical practice, I've treated over 500 patients with type 2 diabetes and prediabetes. Nearly every one tells the same story: years of endocrinologist visits, fasting glucose tests, HbA1c checks, metformin prescriptions.
This is like diagnosing heart failure without measuring blood pressure. Blood sugar is a consequence. HOMA-IR reveals the cause: how much your cells resist insulin. And that determines whether the disease can be reversed.
What Is HOMA-IR and How Is It Calculated
HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) is a mathematical model developed at Oxford University in 1985. The formula is simple:
HOMA-IR = (fasting insulin × fasting glucose) / 22.5
Insulin is measured in μIU/mL, glucose in mmol/L. If glucose is in mg/dL, the formula becomes: (insulin × glucose) / 405.
You need just two tests drawn from the same blood sample, taken in the morning after an overnight fast: insulin and glucose. Cost: typically $15-30 at most labs. Results within 1-2 days.
What Is a Normal HOMA-IR
How to interpret your results:
- Below 1.0 — excellent insulin sensitivity
- 1.0–1.5 — normal range
- 1.5–2.5 — early insulin resistance, the "gray zone"
- 2.5–4.0 — moderate insulin resistance (prediabetes territory)
- Above 4.0 — significant insulin resistance (high diabetes risk or existing diabetes)
In my practice, the average HOMA-IR in newly presenting type 2 diabetes patients is 5.8. For those with prediabetes — 3.4. Notably, many of them still had fasting glucose in the "normal" range of 90-100 mg/dL (5.0-5.5 mmol/L).
Why HbA1c Is Not Enough
HbA1c is the standard marker for diabetes management. It reflects average blood sugar over 3 months. The problem: HbA1c rises late in the disease process.
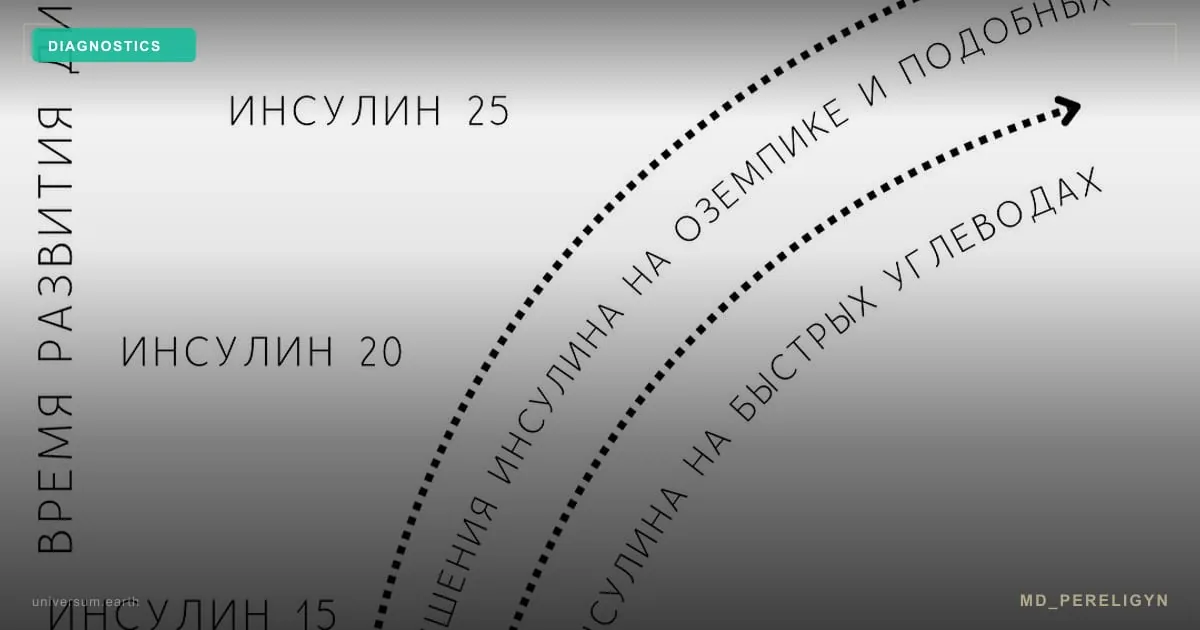
Here's the typical timeline of type 2 diabetes development:
Years 0-5: Insulin resistance builds. HOMA-IR climbs from 1.5 to 3.0. Fasting insulin is elevated (15-25 μIU/mL). Fasting glucose is normal. HbA1c is normal. The patient knows nothing.
Years 5-8: HOMA-IR reaches 3.0-5.0. Fasting glucose starts rising (100-125 mg/dL). HbA1c hits 5.7-6.4% — prediabetes. Doctor says: "Lose weight, come back in six months."
Year 8+: The pancreas becomes exhausted. Insulin production falls. Glucose exceeds 126 mg/dL. HbA1c surpasses 6.5%. Diagnosis: type 2 diabetes. Metformin prescribed.
See the problem? HOMA-IR could have caught the disease at stage one — 5-8 years before diagnosis. But no one ordered it.
Why Doctors Don't Order HOMA-IR
There are several reasons, and they're systemic:
1. Not in standard protocols. Clinical guidelines from the ADA (American Diabetes Association) and most national endocrinology associations don't include fasting insulin and HOMA-IR in routine screening. The doctor follows the protocol — no test ordered.
2. The "treat the sugar" paradigm. Traditional endocrinology focuses on glycemic control. Lower the sugar — mission accomplished. What happens with insulin resistance along the way goes untracked.
3. No drug "for HOMA-IR." If a doctor finds elevated HOMA-IR, what do they prescribe? There's no standard pharmaceutical response. Metformin partially reduces resistance but doesn't eliminate it — see the head-to-head comparison of berberine vs metformin for a closer look at the trade-offs. A comprehensive approach — nutrition, supplements, lifestyle — is needed. Most endocrinologists lack the time and expertise for this.
4. Appointment time. A typical clinic visit is 12-15 minutes. Explaining what HOMA-IR is, why it matters, and how to interpret it — there's simply no time.
What HOMA-IR Tells You About Your Health
HOMA-IR isn't just a diabetes marker. Insulin resistance underlies a whole spectrum of conditions:
- Obesity, especially abdominal (visceral fat)
- Hypertension — insulin promotes sodium retention, raising blood pressure
- Dyslipidemia — high triglycerides, low HDL
- Fatty liver disease (NAFLD) — affects up to 70% of people with insulin resistance
- Polycystic ovary syndrome (PCOS) — insulin resistance is found in 70-80% of women with PCOS
- Increased cardiovascular risk — insulin resistance is an independent risk factor for heart attack and stroke
One test — and you see the root cause behind a dozen different diagnoses.
Clinical Case: Andrew, 47 Years Old
Andrew came to me complaining of fatigue and weight gain (+26 lbs over 2 years). His GP said: "Your labs are normal, just eat less."
The "normal" results: fasting glucose 95 mg/dL (5.3 mmol/L), HbA1c 5.5%. Technically, within range.
I ordered an expanded panel:
- Fasting insulin: 22.4 μIU/mL (normal up to 8)
- HOMA-IR: 5.3 (normal up to 1.5)
- C-peptide: 4.1 ng/mL (upper range)
- Triglycerides: 248 mg/dL (elevated)
- ALT: 52 U/L (elevated — sign of fatty liver)
The picture was clear: significant insulin resistance with compensatory hyperinsulinemia. His pancreas was working 3x harder than normal to keep blood sugar stable. Without intervention — diabetes within 2-3 years.
After 4 months on the md_pereligyn protocol: HOMA-IR dropped to 1.8, insulin to 7.2 μIU/mL, weight decreased by 24 lbs, ALT normalized. Andrew avoided the diabetes that "normal" tests couldn't see.
How to Check Your HOMA-IR
The process is straightforward:
Step 1. Go to any lab and order two tests: fasting insulin and fasting glucose. Both must be drawn from the same blood sample in the morning, after 8-12 hours without food.
Step 2. Calculate HOMA-IR using the formula: (insulin × glucose in mmol/L) / 22.5. Or use any online HOMA-IR calculator.
Step 3. Interpret the result. If HOMA-IR is above 2.5 — you have insulin resistance that needs attention. Above 4.0 — this is a serious issue requiring immediate action.
Step 4. Complete the picture: C-peptide, lipid panel, ALT/AST, hs-CRP, vitamin D, magnesium. These tests reveal the full extent of metabolic dysfunction and help build a correction plan.
Can You Lower HOMA-IR
Yes — and this is the greatest value of this index: it's reversible. In my practice:
- Average HOMA-IR at intake: 5.8
- Average HOMA-IR after 3-4 months on protocol: 1.9
- 85% of patients achieve HOMA-IR below 2.5 (exiting the insulin resistance zone)
What works to lower HOMA-IR:
Nutrition: reduce refined carbohydrates, increase protein and healthy fats, eat within an 8-10 hour window.
Targeted supplements: berberine (900-1500 mg/day), magnesium glycinate (200-400 mg), chromium picolinate (500 mcg), omega-3 (2-4 g). All have evidence for reducing HOMA-IR — see the full evidence review of the best supplements for insulin resistance for dosing and study data.
Physical activity: walking after meals (15-20 min), resistance training 2-3 times per week. Muscle mass is the body's largest glucose consumer.
Sleep: 7-8 hours in darkness. A single night of sleep deprivation increases insulin resistance by 25-30% (Donga et al., 2010, Journal of Clinical Endocrinology & Metabolism).
Your First Step
Order a fasting insulin test. It's one inexpensive test that can change your life. If your HOMA-IR is above 2.5 — don't wait for blood sugar to climb and for a diabetes diagnosis. Act now, while the condition is reversible.
During a consultation, we'll review your labs, determine your stage of insulin resistance, and create a personalized correction plan. 85% of my patients return their HOMA-IR to normal within 3-4 months — the same approach that drove the outcomes documented across 500 patients in diabetes remission. You could be next.