Early CKD (stages 1-2)
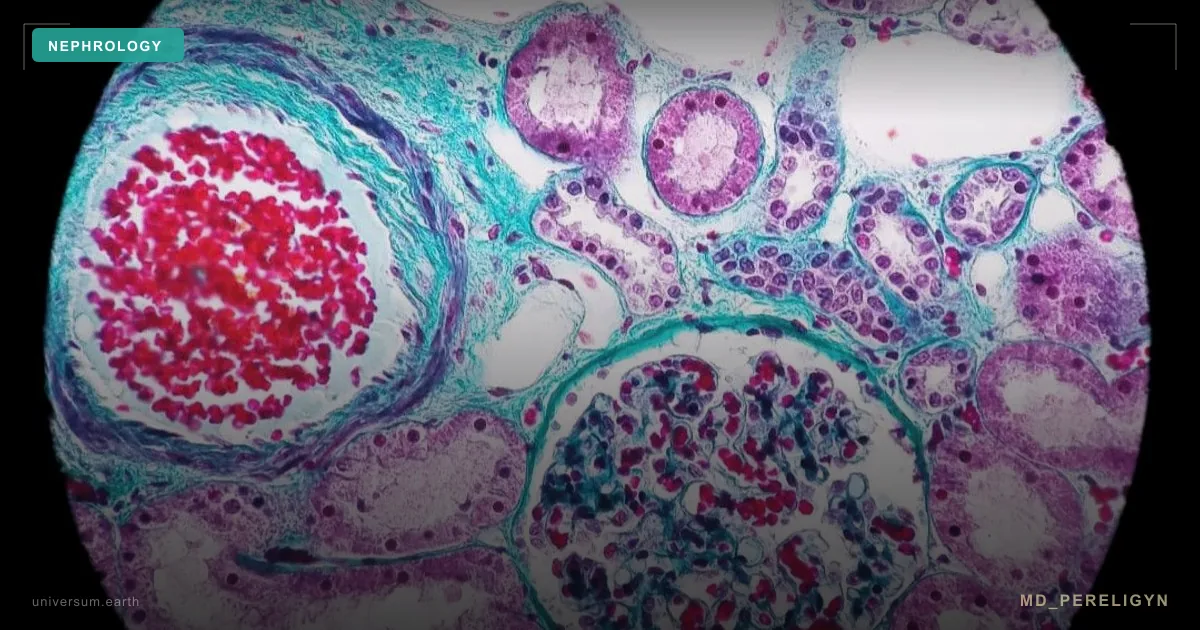
Chronic kidney disease stages 1-2 is defined as persistent (>3 months) GFR reduction to 60-89 mL/min/1.73 m² or normal GFR with markers of damage such as albuminuria or structural abnormalities. Prevalence in the general population reaches 8-10%. Frequently asymptomatic and detected only through systematic screening.