Introduction: why NSAIDs are the most common drug-induced cause of AKI
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first-line over-the-counter analgesics: ibuprofen, diclofenac, naproxen, ketorolac, nimesulide, meloxicam, celecoxib. According to NHANES data, up to 27% of the adult US population takes NSAIDs at least once per week; in EU countries, ibuprofen is among the top 3 best-selling over-the-counter drugs.
At the same time, NSAIDs rank first among drug-induced causes of acute kidney injury (AKI) in adults.
Key point of the md_pereligyn protocol: NSAIDs are not “safe” or “dangerous” by themselves; they become dangerous in combination with risk factors: age 65+, dehydration, ACE inhibitor/ARB + diuretic, and concomitant CKD. A short course (≤10 days) in a healthy adult is almost always tolerated. Chronic use without eGFR monitoring is the main mechanism of iatrogenic stage 3 CKD.
🌀
Three Mechanisms of Kidney Damage
NSAIDs damage the kidney not through one pathway, but through three independent pathways, each with its own clinical scenario, time course, and set of markers.
▸Mechanism 1 — hemodynamic (prerenal) AKI. NSAIDs block COX-1/COX-2-dependent synthesis of vasodilatory prostaglandins (PGE2, PGI2) in the afferent arteriole of the glomerulus. Vasoconstriction occurs, renal blood flow falls, and GFR decreases. In a dehydrated patient (vomiting, diarrhea, heat exposure, marathon) or in a patient taking an ACE inhibitor/ARB + diuretic, this produces classic prerenal AKI within the first 24–72 hours of use. ▸Mechanism 2 — acute allergic interstitial nephritis (AIN). An immune-mediated reaction to an NSAID or metabolite. The classic triad of “fever + rash + eosinophilia” occurs in less than 10% of cases; in most cases, AIN is clinically silent. It develops during weeks 2–8 of use, more often with selective COX-2 inhibitors and in combination with PPI. The marker is eosinophiluria on urinalysis. ▸Mechanism 3 — chronic analgesic nephropathy with papillary necrosis. This develops with a cumulative NSAID dose of more than 1–2 kg over a lifetime (approximately 10 tablets of ibuprofen 400 mg daily for 3+ years). Combination analgesics are especially dangerous (phenacetin-containing drugs historically; acetaminophen + caffeine + codeine in modern over-the-counter forms). It progresses to stage 4–5 CKD over 10–15 years.
These three mechanisms require different prevention strategies and different monitoring frequency.
🌀
Drivers of Damage
Eight factors, each of which independently increases the risk of NSAID-induced AKI by 50–200%. In combination, the effect is multiplicative.
•Age over 65 years — reduced baseline renal perfusion, narrow tubular reserve, and frequent polypharmacy. The risk of AKI on NSAIDs increases 2–4-fold compared with younger patients. •Dehydration — vomiting, diarrhea, heat, prolonged endurance training, fluid restriction before surgery. Prerenal mechanism 1 is triggered even with minimal reduction in circulating blood volume. •Triple hit — NSAID + (ACE inhibitor or ARB) + loop diuretic increases AKI risk threefold compared with one NSAID tablet alone (Lapi F, BMJ 2013, PMID 23299844[1]). This combination should be avoided in all patients 65+. •Concomitant stage 3 or higher CKD — eGFR 30–60 mL/min — a narrow therapeutic window; any vasoconstriction of the afferent arteriole produces a measurable decrease in GFR. •Liver cirrhosis, heart failure, nephrotic syndrome — prerenal states with occult hypovolemia; NSAIDs are contraindicated in these patients. •Concurrent proton pump inhibitors (PPI) — increase the risk of AIN by 1.5–2 times when combined with NSAIDs. •Diabetes mellitus with diabetic nephropathy — the combination of microangiopathy and NSAID-induced vasoconstriction leads to accelerated progression. •High doses and combination formulations — fixed combinations such as diclofenac + misoprostol and acetaminophen + codeine + caffeine make it harder to control cumulative dose.
🌀
Which NSAIDs Are Safer (and Which Are Not)
Within the NSAID class, there are substantial differences in nephrotoxicity. Ranking based on large cohorts and meta-analyses:
| Drug | Limit |
|---|---|
| Ibuprofen | ≤1200 mg/day |
| Naproxen | ≤500 mg/day |
| Diclofenac | >100 mg/day — high risk |
| Ketorolac | >5 days — high risk |
| Acetaminophen | ≤3 g/day — safe |
▸Relatively safer (short course): ibuprofen (≤1200 mg/day), naproxen (≤500 mg/day). With short duration (≤10 days) in a healthy adult without risk factors, nephro-safety is acceptable. ▸Intermediate risk: meloxicam (7.5–15 mg/day), celecoxib (200 mg/day). COX-2 selectivity reduces gastrointestinal risk, but does not reduce renal risk: prostaglandin regulation of the afferent arteriole is mediated through COX-2. ▸High risk: diclofenac (especially at doses >100 mg/day), ketorolac (>5 days of use), indomethacin, nimesulide, ketoprofen. These drugs show the highest risk of AKI and cardiovascular events in cohort data. ▸Paradox: the belief that “selective COX-2 inhibitors are safer for the kidneys” is a myth. They are safer for the stomach (fewer erosions and bleeding events), but renal risk is comparable or higher because of more pronounced COX-2 blockade in the kidney.
The safest strategy for chronic pain is to avoid systemic NSAIDs and use topical formulations (see protocol below).
🌀
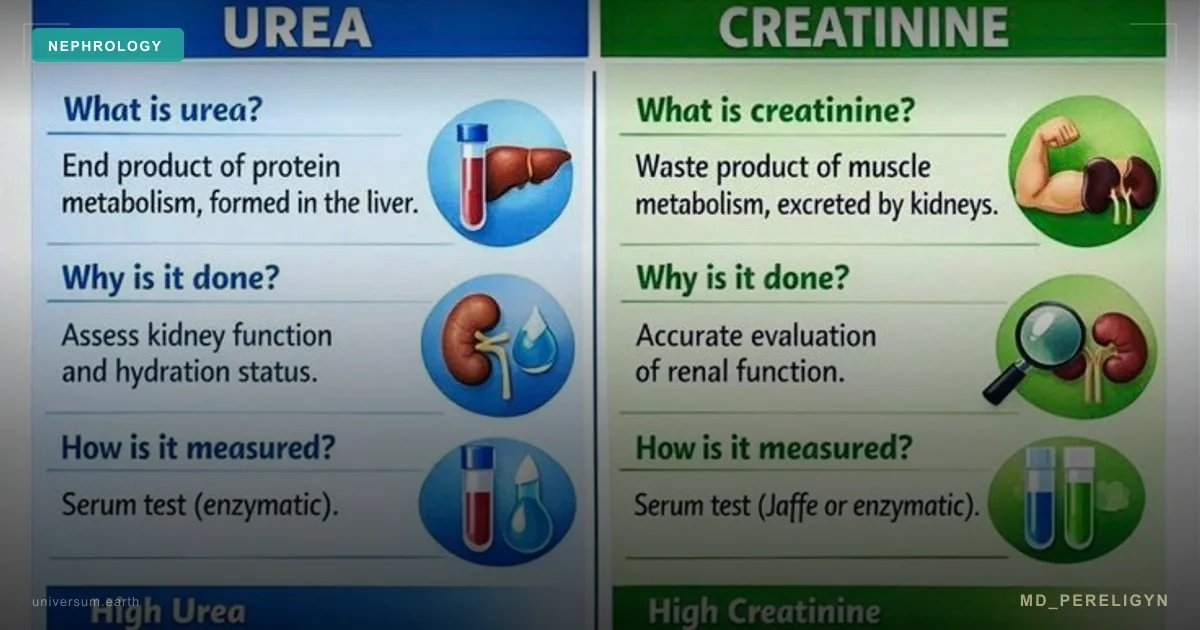
Early Biomarkers of Damage
NSAID-induced AKI is often asymptomatic and detected only through laboratory monitoring. What to monitor:
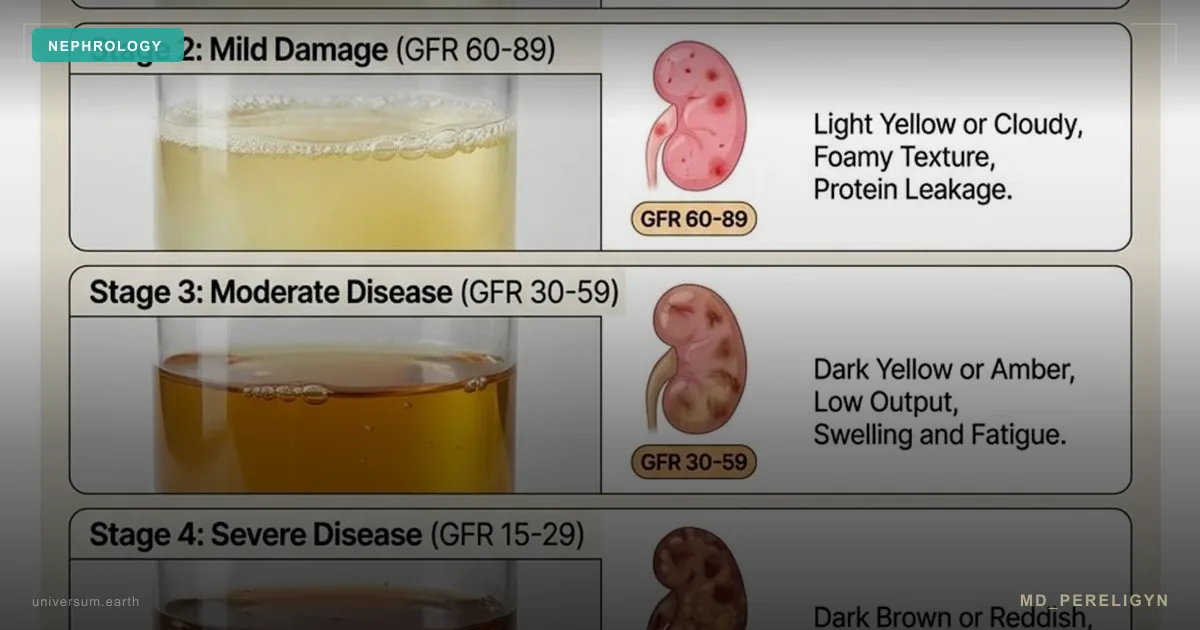
▸Creatinine increase of more than 26 μmol/L within 48 hours — the KDIGO criterion for stage 1 AKI. In a patient 65+ on an NSAID course, this is a marker for immediate discontinuation (KDIGO 2024, Kidney Int Suppl). ▸eGFR decrease of more than 25% from baseline during the first 7–14 days of use — a reason to discontinue and find an alternative. ▸Serum potassium above 5.0 mmol/L — hyperkalemia caused by reduced distal sodium-potassium exchange; especially dangerous when combined with ACE inhibitors/ARBs. ▸Eosinophiluria greater than 1% on urinalysis — a surrogate marker of acute interstitial nephritis. ▸Fractional excretion of sodium (FENa) below 1% — distinguishes prerenal AKI (mechanism 1) from tubular necrosis. ▸New proteinuria or microhematuria during NSAID use — a reason for nephrology consultation. ▸Urine output below 0.5 mL/kg/hour for 6 hours — the clinical criterion for oliguria and an early sign of AKI.
Minimum monitoring for patients 65+ or with risk factors: creatinine and potassium before starting an NSAID course, after 7–10 days, and after 4 weeks if use continues.
🌀
Holistic Protocol for Safe Use
The principle of the md_pereligyn protocol: NSAIDs are a temporary tool for acute pain, not a baseline strategy for chronic pain. In a patient with chronic pain, the task is to find and address the cause (often systemic inflammation, visceral fat, dysbiosis), not to mask it with daily ibuprofen.
1. Dose and Duration Limits
▸Course no longer than 10 days without reassessing creatinine and potassium. ▸Ibuprofen ≤1200 mg/day, naproxen ≤500 mg/day as a reasonable ceiling for over-the-counter use. ▸Diclofenac ≤75 mg/day and only as a short course (≤5–7 days) in patients under 65 years without risk factors. ▸Ketorolac ≤5 days — this is an absolute limit; beyond 5 days, AKI risk rises nonlinearly.
2. Complete Discontinuation in Risk Situations
▸Discontinue 72 hours before planned surgery — reduces the risk of perioperative AKI and bleeding. ▸Avoid the combination of NSAID + (ACE inhibitor or ARB) + diuretic in patients 65+. If analgesia is needed, use acetaminophen or topical NSAIDs. ▸Discontinue during acute gastroenteritis, vomiting, diarrhea, or heat exposure — even in a young patient, dehydration makes prerenal mechanism 1 dangerous. ▸Complete avoidance in stage 4–5 CKD (eGFR <30) — NSAIDs are contraindicated.
3. Alternatives for Chronic Pain
▸Acetaminophen up to 3 g/day as first-line therapy for chronic nociceptive pain. With normal liver function and no chronic alcohol use, it is nephro-safe. ▸Topical NSAID gels (diclofenac gel, ibuprofen gel) — systemic bioavailability is less than 5%. Effective for osteoarthritis of large joints, muscle pain, and postoperative localized pain. ▸Capsaicin cream 0.025–0.075% — for neuropathic pain and osteoarthritis; zero systemic burden. ▸Duloxetine 30–60 mg/day — for chronic musculoskeletal pain with a depressive/anxiety component. ▸Gabapentin 900–2400 mg/day or pregabalin 150–600 mg/day — for neuropathic pain. ▸A mild muscle relaxant (tizanidine 2–4 mg at night) — for a muscle-spastic component.
4. Holistic Anti-Inflammatory Strategies
▸Course hydration of 30 mL/kg body weight per day when prescribing an NSAID course — reduces the risk of prerenal AKI. ▸Omega-3 EPA+DHA 2–3 g/day — lowers the systemic inflammatory background; in some patients with osteoarthritis, it reduces NSAID need by 30–50%. ▸Curcumin (with piperine or liposomal) 500–1000 mg twice/day — meta-analyses in osteoarthritis show an effect comparable to ibuprofen 800 mg/day, without nephrotoxicity. ▸Boswellia (AKBA-standardized extract) 100–300 mg/day — a selective 5-LOX inhibitor; an alternative for osteoarthritis. ▸Reduction of visceral fat — every −5 kg of body weight in obesity reduces knee joint load 4-fold (biomechanical multiplication). ▸Therapeutic exercise and strength training — quadriceps strengthening in knee osteoarthritis reduces pain and NSAID need twofold. ▸Adequate sleep 7–9 hours — sleep deprivation increases inflammatory cytokines (IL-6, TNF-α) and the pain threshold.
5. Monitoring During Chronic Use
▸If NSAIDs are needed chronically — creatinine, potassium, eGFR every 3 months. ▸Microalbuminuria once every 6 months — an early marker of tubular injury. ▸Urinalysis for eosinophiluria at the first suspicion of AIN (unexplained eGFR decline, minimal rash, fatigue).
🌀
What Does NOT Work (and Why)
▸PPI “stomach protection” does not protect the kidney — PPI reduce gastrointestinal risk, but not renal risk; moreover, the NSAID + PPI combination itself increases the risk of acute interstitial nephritis. ▸“Safe” nimesulide — a myth. The drug is banned or restricted in Finland, Spain, Belgium, and Ireland because of hepato- and nephrotoxicity. ▸Replacing a systemic NSAID with “mild” aspirin at 100 mg/day “for pain relief” — low-dose aspirin has no analgesic effect but increases bleeding risk. ▸Acetaminophen + NSAID continuously — the combination of acetaminophen + ibuprofen for a short period (≤3 days) is acceptable, but chronic daily use is equivalent to a higher NSAID dose with the same risks. ▸Homeopathic “nonsteroidals” and “herbal anti-inflammatories” — most (Wobenzym, serrapeptase at usual doses) have no proven clinical effect on chronic pain; they do not replace NSAIDs and do not provide analgesia. ▸Opioids as a “safe” alternative in CKD — codeine and tramadol are metabolized by the kidneys; in stage 4–5 CKD, they accumulate with overdose risk.
🌀
When to Seek Care
▸Chronic pain (≥3 months) requiring daily NSAID use ▸Age 65+ and NSAID use without eGFR monitoring during the last 12 months ▸Combination of NSAID + ACE inhibitor/ARB + diuretic in current therapy ▸Concomitant stage 3 or higher CKD + pain episodes requiring analgesia ▸An episode of unexplained creatinine rise during an NSAID course ▸Suspicion of acute interstitial nephritis (unexplained eGFR decline, eosinophiluria, minimal rash) ▸Desire to switch from chronic NSAIDs to a safe multimodal protocol
I perform a complete nephrology screening (creatinine, eGFR, cystatin C, microalbuminuria, urinalysis, electrolytes, uric acid), review the current analgesic regimen, and create a personalized multimodal protocol with minimal renal burden.
🌀
Conclusion
NSAIDs are a scalpel, not a pillow. A short course (≤10 days) in a healthy adult without risk factors is acceptably safe. Chronic daily use, especially in patients 65+ or in combination with ACE inhibitor/ARB + diuretic, is a pathway to iatrogenic stage 3 CKD over 10–15 years.
A harmless ibuprofen tablet damages the kidney more often than creatinine in a blood test warns you about it. One 10-day course is safe; ten courses per year without eGFR monitoring is a pathway to stage 3 CKD within a decade.
Chronic pain requires searching for the cause, not masking the symptom. A holistic protocol — multimodal analgesia, topical formulations, omega-3, curcumin, weight reduction, strength training — provides sustained pain reduction without a renal cost.
🌀
Sources
▸Lapi F, Azoulay L, Yin H, et al. Concurrent use of diuretics, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers with non-steroidal anti-inflammatory drugs and risk of acute kidney injury: nested case-control study. BMJ 2013;346:e8525. PMID 23299844 ▸KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl 2024.
Related articles: Endothelium: the Foundation of Vascular Health, Cholesterol Without Statins.
🌀
FAQ
Can I take ibuprofen for a cold if I am generally healthy? Yes, a short course (3–5 days) of ibuprofen 400 mg 3 times/day in a healthy adult without risk factors is safely tolerated. Conditions: adequate hydration (1.5–2 L of water/day), no vomiting/diarrhea, and no concomitant ACE inhibitors/ARBs/diuretics. With marked fever and sweating, prefer acetaminophen to avoid combining NSAIDs with dehydration.
My grandmother is 78 years old and has knee arthritis; she takes diclofenac constantly. Is that dangerous? Extremely dangerous. A 78-year-old patient is very likely to already have reduced baseline eGFR (60–80 mL/min), and chronic diclofenac is one of the most nephrotoxic NSAIDs. Urgently check: creatinine, eGFR, potassium. Replace with: topical diclofenac gel + acetaminophen 3 g/day + capsaicin cream + quadriceps exercise therapy. If the effect is insufficient — duloxetine 30 mg.
Is acetaminophen safe for the kidney with long-term use? Yes, at a dose of ≤3 g/day, with normal liver function and no chronic alcohol use, acetaminophen is nephro-safe. Older data on “phenacetin nephropathy” referred to phenacetin (an acetaminophen precursor withdrawn from the market in the 1980s), not to acetaminophen itself. Modern large cohorts (NHANES, UK Biobank) do not confirm a clinically significant renal risk from acetaminophen monotherapy at therapeutic doses.
What should I do if creatinine jumped after an NSAID course? (1) Stop the NSAID immediately. (2) Hydration 30 mL/kg/day (if there are no contraindications). (3) Check creatinine and potassium after 48 and 72 hours. (4) Stop or adjust ACE inhibitors/ARBs/diuretics together with the treating physician. (5) If creatinine does not return to baseline within 5–7 days or continues to rise — nephrology consultation and urinalysis for eosinophiluria (to rule out AIN).
What are the alternatives to NSAIDs for osteoarthritis of large joints? A multimodal protocol: (1) topical diclofenac gel 4 times/day, (2) acetaminophen 3 g/day, (3) curcumin with piperine 1000 mg 2 times/day, (4) omega-3 EPA+DHA 2–3 g/day, (5) a strength program for quadriceps/gluteal muscles 3 times/week, (6) weight reduction if BMI >27. If the effect is insufficient — intra-articular hyaluronic acid or PRP; in severe knee osteoarthritis — discussion of joint replacement with an orthopedic surgeon. Systemic NSAIDs are last-line, not first-line.
This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.
🌀
Acetaminophen as the principal NSAID alternative: mechanism and the dose ceiling that preserves renal safety
The original article correctly names acetaminophen (paracetamol) as the first-line analgesic alternative in renal risk groups but does not explain why its renal profile differs from NSAIDs or where the safety advantage breaks down. The distinction matters because acetaminophen's reputation as "renally safe" is dose-dependent and not absolute.
Mechanism. Acetaminophen inhibits central prostaglandin synthesis primarily through a peroxidase-dependent pathway, with relatively weak effect on the peripheral COX-1 and COX-2 isoenzymes that maintain renal afferent arteriolar vasodilation. At therapeutic doses, intrarenal prostaglandin production is preserved, glomerular perfusion is not compromised, and the medullary thick ascending limb retains its sodium and water reabsorptive capacity. This is the structural reason it is preferred in CKD, heart failure, cirrhosis, and elderly patients with borderline volume status.
Dose ceiling for renal safety. The threshold at which acetaminophen begins to behave like an NSAID toward the kidney is approximately 3 g/day chronically or 4 g/day acutely. Above these thresholds, two mechanisms emerge. First, the reactive metabolite N-acetyl-p-benzoquinone imine (NAPQI) accumulates in renal tubular cells once hepatic glutathione is depleted, producing a delayed acute tubular injury phenotype that lags 48–72 hours behind hepatotoxicity.
Practical prescribing in renal risk patients. Use 500 mg every 6 hours as the default starting regimen; this is 2 g/day, comfortably below both ceilings. Reserve 1,000 mg every 6 hours (4 g/day) for ≤3 days of moderate pain. In eGFR <30 or active liver disease, cap chronic daily intake at 2 g/day and extend the dosing interval to 8 hours. Always reconcile with combination products: many over-the-counter cold preparations, opioid co-formulations, and migraine medications contain 325–500 mg of acetaminophen per dose and account for most inadvertent overdoses.
Specific contraindications independent of renal status. Chronic alcohol use exceeding 3 standard drinks daily, fasting states beyond 24 hours, malnutrition, and concurrent isoniazid or rifampin therapy all reduce hepatic glutathione and lower the toxic threshold by approximately 30–50%. In these contexts, 2 g/day is the effective ceiling regardless of measured eGFR.
What acetaminophen does not replace. Acetaminophen has no anti-inflammatory action at peripheral tissues at clinical doses. For inflammatory arthropathies, gout flares, or post-traumatic edema, the analgesic effect is partial and patients often escalate dosing in a way that breaches the renal-safety ceiling. In those scenarios, topical diclofenac, short-course oral NSAIDs with full risk-stratification, or non-pharmacologic measures should be considered before chronic acetaminophen above 2 g/day.
References
- PMID 23299844. PMID 23299844