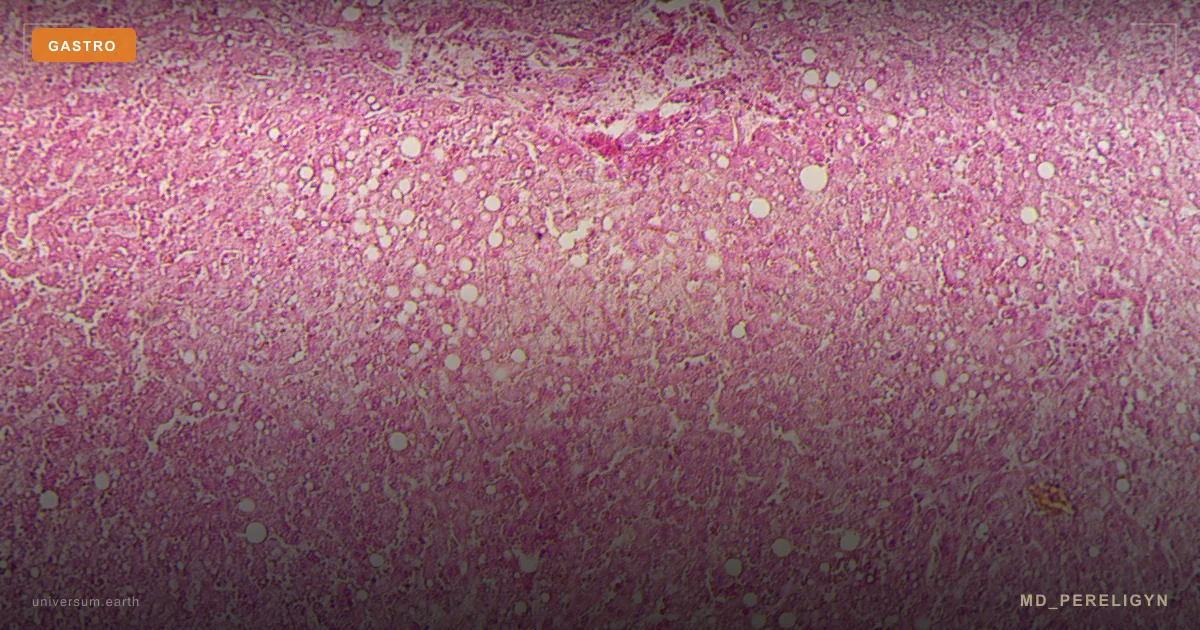
H. pylori gastritis
Chronic gastric mucosal inflammation caused by Helicobacter pylori, a gram-negative microaerophilic bacterium. Diagnostic threshold: positive urea breath test, stool antigen, or histology. Global prevalence is approximately 44%, higher in developing regions. Key features: epigastric pain, dyspepsia, increased risk of peptic ulcer and MALT lymphoma with long-term persistence.