What Is Glutathione and Why It Matters
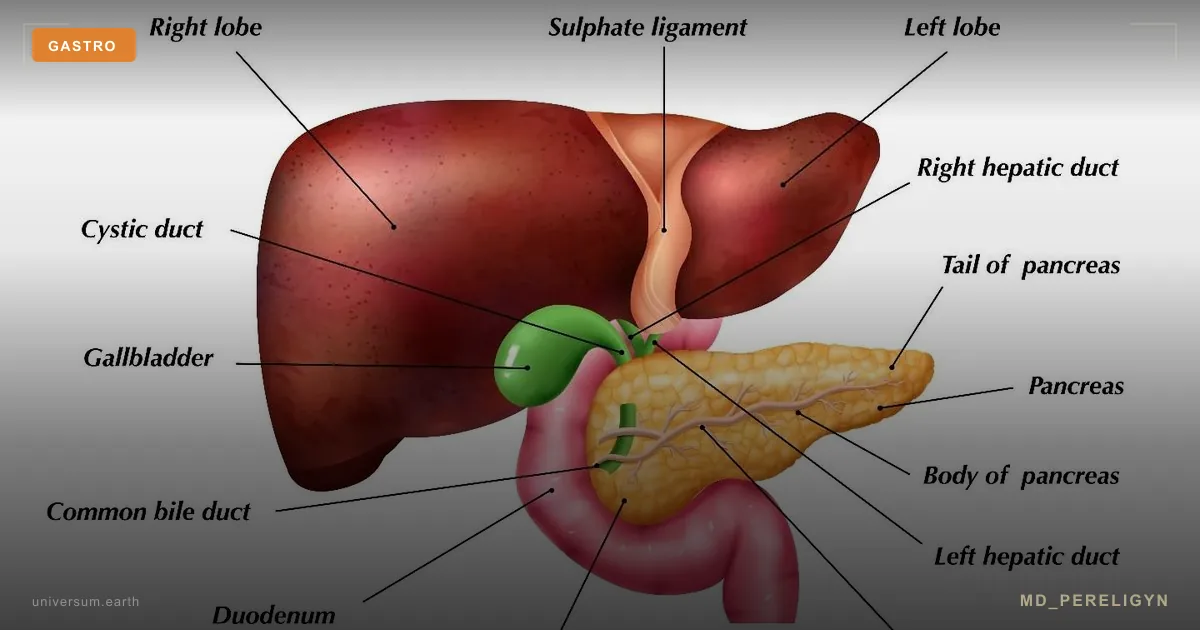
Glutathione (GSH) is a tripeptide composed of three amino acids: glutamic acid, cysteine, and glycine. It is present in every cell, but the liver contains the highest concentrations — up to 5-10 mM. According to a comprehensive review in Antioxidants & Redox Signaling (2018), glutathione is the most potent intracellular antioxidant and plays a central role in maintaining redox homeostasis.
The key indicator of cellular health is the ratio of reduced glutathione (GSH) to oxidized glutathione (GSSG). In healthy cells, this ratio is approximately 100:1. Under oxidative stress, toxic exposure, chronic inflammation, or aging, the balance shifts toward GSSG, triggering lipid peroxidation, DNA damage, and apoptosis.
The Three Phases of Hepatic Detoxification
Phase I: Oxidation (Cytochrome P450 System)
The cytochrome P450 (CYP450) enzyme family serves as the liver's first line of defense. These enzymes perform oxidation, reduction, and hydrolysis reactions, converting fat-soluble toxins into more reactive intermediate metabolites. CYP3A4, CYP2D6, CYP1A2, and CYP2C9 are the primary isoforms, collectively metabolizing up to 80% of all pharmaceutical drugs (Annual Review of Pharmacology and Toxicology, 2018).
The Phase I paradox: intermediate metabolites are often more toxic than the parent compounds. They generate free radicals that damage hepatocyte membranes. This is precisely why Phase II must operate in synchrony with Phase I — any imbalance creates a dangerous accumulation of reactive intermediates.
Phase II: Conjugation
Reactive intermediates from Phase I are bound to endogenous molecules, becoming water-soluble and less toxic. Key conjugation reactions include: glutathione S-transferase (GST) conjugation, glucuronidation (UGT), sulfation (SULT), methylation (COMT, TPMT), acetylation (NAT), and amino acid conjugation (glycine, taurine).
GST conjugation is one of the most critical Phase II reactions. The GST enzyme couples glutathione with electrophilic metabolites, neutralizing them. A meta-analysis in PLoS ONE (2014) showed that polymorphisms in GSTM1 and GSTT1 genes (null genotypes) are associated with increased cancer risk due to reduced detoxification capacity.
Phase III: Elimination (Transport)
Conjugated metabolites must be efficiently exported from the cell. Phase III is mediated by ABC (ATP-binding cassette) transporter proteins: P-glycoprotein (MDR1/ABCB1), MRPs (multidrug resistance-associated proteins), and BCRP. These transporters pump conjugates into bile (for intestinal excretion) or blood (for renal excretion).
Phase III dysfunction leads to intracellular accumulation of conjugated toxins — a mechanism underlying drug-induced liver injury. Research in Hepatology (2019) demonstrated that genetic variants of ABCB1 and ABCC2 transporters significantly affect elimination rates.
Why Glutathione Levels Decline
Chronic oxidative stress consumes glutathione faster than cells can regenerate it. Major causes of depletion include: - Chronic infections and inflammation (increased GSH consumption by immune cells) - Heavy metal exposure (mercury, lead, cadmium bind directly to GSH) - Alcohol (acetaldehyde, the toxic metabolite, requires GSH for detoxification) - Acetaminophen/paracetamol (forms NAPQI, neutralized by glutathione) - Aging (after 45, GSH synthesis declines 10-15% per decade) - Precursor deficiency: cysteine, glycine, glutamic acid, selenium, vitamin B6
NAC: The Key Glutathione Precursor
N-acetylcysteine (NAC) is the acetylated form of L-cysteine, which is the rate-limiting factor in glutathione synthesis. NAC has been used clinically for over 50 years: as a mucolytic, as the antidote for acetaminophen overdose, and as a protectant against contrast-induced nephropathy.
A meta-analysis in Advances in Pharmacological Sciences (2019) confirmed that oral NAC (600-1200 mg/day) significantly increases intracellular glutathione levels. A landmark study in Free Radical Biology and Medicine (2011) demonstrated that combining NAC (600 mg) with glycine (100 mg/kg/day) in elderly subjects restored GSH levels to those of young volunteers within just 2 weeks.
Glutathione Forms: Oral, Liposomal, and Intravenous
Standard oral glutathione is poorly absorbed — gastrointestinal peptidases break down the tripeptide into individual amino acids. Bioavailability is approximately 3-5%.
| Form | Note |
|---|---|
| Oral | 3–5% bioavailability |
| Liposomal | +30–35% GSH in 4 weeks |
| Intravenous | 100% bioavailability |
Liposomal glutathione is encapsulated in phospholipid vesicles that protect the molecule from GI degradation. A randomized placebo-controlled trial in the European Journal of Nutrition (2015) demonstrated that liposomal GSH (500-1000 mg/day) increased erythrocyte glutathione stores by 30-35% over 4 weeks.
Intravenous glutathione (IV GSH) provides 100% bioavailability and immediate elevation of plasma levels. Used in integrative clinics for intensive detoxification, neuroprotection, and post-chemotherapy recovery. Typical dose: 600-2400 mg per infusion, administered 1-3 times per week.
The Milano Cocktail is an intravenous formula developed in Italian anti-aging clinics: glutathione 600 mg + vitamin C 5000 mg + alpha-lipoic acid 600 mg + B-complex vitamins. The combination provides synergistic antioxidant and detoxification effects by recycling glutathione through ascorbic acid and alpha-lipoic acid.
Glutathione Restoration Protocol
Foundation Protocol (daily): - NAC: 600 mg twice daily on an empty stomach - Glycine: 3-5 g/day (can be taken before bed — improves sleep quality) - Selenium (selenomethionine): 200 mcg/day — cofactor for glutathione peroxidase - Vitamin C: 1000 mg twice daily — recycles oxidized GSSG back to GSH - Alpha-lipoic acid (R-form): 300-600 mg/day — universal antioxidant that regenerates GSH
Advanced Protocol (confirmed deficiency): - Liposomal glutathione: 500-1000 mg in the morning on an empty stomach - Milk thistle (silymarin): 420 mg/day — stimulates GSH synthesis in hepatocytes (Hepatology, 2010) - Sulforaphane (broccoli extract): 50-100 mg/day — activates the Nrf2 pathway, upregulating glutathione synthesis genes - S-adenosylmethionine (SAMe): 400-800 mg/day — methyl donor, supports Phase II methylation reactions
Diagnostic Assessment
- Erythrocyte glutathione (GSH/GSSG ratio) — the most accurate marker of intracellular stores - Organic Acids Test (OAT) — pyroglutamic acid is elevated in GSH deficiency - 8-OHdG — marker of oxidative DNA damage - Genetic testing — GSTM1, GSTT1, GSTP1, GPX1 polymorphisms determine individual requirements
Frequently Asked Questions
Can diet alone raise glutathione levels? Partially. Foods rich in sulfur-containing amino acids (eggs, garlic, cruciferous vegetables, onions) support GSH synthesis. However, with confirmed deficiency, diet alone is insufficient — targeted supplementation is needed.
NAC or liposomal glutathione — which is better? NAC is a precursor the body uses to synthesize its own GSH. Liposomal glutathione is the preformed molecule. For a long-term strategy, the optimal approach is combining daily NAC with periodic liposomal GSH courses.
Is NAC safe for asthma patients? Use with caution. High doses of NAC (>1800 mg/day) may trigger bronchospasm in some asthma patients. Start with 600 mg/day and titrate.
How often should IV glutathione be administered? Standard course: 1-2 times per week for 4-8 weeks. Maintenance: once every 2-4 weeks. Always under physician supervision.
Does alcohol affect glutathione levels? Significantly. Even moderate consumption (2-3 drinks) reduces hepatic GSH by 20-30%. Regular drinking creates chronic GSH deficiency, accelerating the development of alcoholic liver disease.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before starting any treatment protocol.
🌀
Genotype-Stratified Interpretation of Detoxification Polymorphisms
The article recommends testing GSTM1, GSTT1, GSTP1, and GPX1 polymorphisms but does not describe how the genotype alters management. Each variant has measurable functional consequences that justify specific intervention emphasis.
GSTM1 null (deletion) is present in approximately 40–50% of European populations and up to 60% of East Asian populations. Carriers have absent GSTM1 enzyme activity, reducing conjugation capacity for polycyclic aromatic hydrocarbons, benzene metabolites, and several chemotherapy agents. Meta-analyses show GSTM1-null carriers have an increased risk of bladder cancer, lung cancer in smokers, and worse outcomes with platinum-based chemotherapy. For these patients, environmental exposure reduction — air filtration, water filtration, and avoidance of grilled or smoked meats — has higher yield than supplement intensification.
GSTT1 null occurs in 15–25% of European and 35–60% of Asian populations. Carriers have impaired conjugation of small reactive metabolites including dichloromethane, ethylene oxide, and certain therapeutic alkylating agents. Combined GSTM1/GSTT1 null genotype magnifies risk; these individuals should avoid solvent occupational exposure and benefit disproportionately from cruciferous-vegetable-derived sulforaphane, which upregulates compensatory Nrf2-driven enzymes.
GSTP1 Ile105Val (rs1695) alters substrate specificity and is associated with reduced activity for hydrophobic electrophiles. Val/Val homozygotes have attenuated response to oxidative stress but, paradoxically, sometimes better response to specific chemotherapies because tumor cells share the deficit. Clinical relevance is highest in patients with concurrent inflammatory disease or NAFLD.
GPX1 Pro198Leu (rs1050450) reduces glutathione peroxidase activity by approximately 30% in Leu/Leu carriers and is associated with cardiovascular and oncologic risk. Selenium status becomes rate-limiting: targeting plasma selenium of 120–150 µg/L through selenomethionine 200 µg/day is more effective in these carriers than in wild-type individuals.
Genotyping does not replace functional assessment; it stratifies the risk-benefit ratio of intensified intervention. A patient with normal GSH/GSSG, normal 8-OHdG, and GSTM1-null genotype does not require aggressive supplementation — only sustained exposure avoidance.
🌀
Monitoring Schedule, Stopping Rules, and Safety Endpoints
A protocol without follow-up is incomplete. NAC and IV glutathione protocols require structured monitoring because both efficacy and toxicity are dose- and duration-dependent.
NAC at 600–1200 mg/day: Baseline labs should include complete blood count, comprehensive metabolic panel, GGT, and homocysteine. Reassess at 8 and 12 weeks. NAC reduces homocysteine through cysteine donation but can transiently raise it in patients with B12 or folate deficiency, so methylation status must be corrected concurrently. Stop NAC if the patient develops bronchospasm or persistent nausea.
IV glutathione 600–2400 mg, 1–3 times weekly: Pre-infusion checks should include electrolytes (especially for the Milano cocktail containing vitamin C 5 g, which can precipitate calcium oxalate stones in predisposed patients), creatinine, and a G6PD screen in patients of Mediterranean, African, or Southeast Asian ancestry. High-dose ascorbate in G6PD-deficient individuals can precipitate hemolytic crisis. Discontinue IV protocols if liver enzymes rise above 2× baseline or if the patient develops sulfur-related odor intolerance, headache, or hypotension during infusion.
Alpha-lipoic acid 300–600 mg/day: Monitor glycemia. ALA improves insulin sensitivity and may precipitate hypoglycemia in patients on sulfonylureas or insulin. Thiamine status should be checked at baseline and every 3 months in long-term users — ALA can deplete thiamine and trigger neuropathy paradoxically resembling the deficit it was given to correct.
Endpoint criteria for protocol success: erythrocyte GSH rises above 1000 µmol/L; GSH/GSSG ratio above 100:1; 8-OHdG returns to laboratory midrange; pyroglutamic acid normalizes; and the patient reports resolution of the symptom that prompted intervention (fatigue, post-exertional malaise, chemical sensitivity, brain fog). Failure to achieve any biomarker shift after 12 weeks of full protocol indicates either non-adherence, ongoing exposure, or that GSH depletion is downstream rather than primary — at which point the differential outlined in the next section becomes essential.
🌀
Contraindications and Clinically Significant Drug Interactions
The original article briefly mentions caution with NAC in asthma but does not enumerate the broader contraindication set, which is clinically consequential.
NAC contraindications and interactions: Avoid concurrent nitroglycerin — NAC potentiates the hypotensive and headache-inducing effects through enhanced nitric oxide release. Reduce or hold NAC 48 hours before any oncologic chemotherapy unless explicitly approved by the oncologist; NAC may reduce efficacy of cisplatin, doxorubicin, and arsenic trioxide by neutralizing the intended oxidative tumor injury. NAC is contraindicated in active peptic ulcer disease due to gastric irritation, and in patients with a documented sulfa or sulfite hypersensitivity, although true allergic cross-reactivity is uncommon.
Glutathione (oral or IV) contraindications: Active malignancy under treatment is a relative contraindication for the same reason — tumor cells exploit high glutathione for chemoresistance. Discuss with the treating oncologist; some protocols permit pulsed glutathione 48 hours after cytotoxic dosing. Glutathione is contraindicated in patients with a history of severe sulfite reactions. Patients with end-stage renal disease should not receive high-dose IV glutathione without nephrology input because sulfur metabolite clearance is impaired.
Alpha-lipoic acid interactions: Potentiates insulin, sulfonylureas, and GLP-1 agonists — hypoglycemia risk. Chelates divalent cations; separate dosing from levothyroxine, iron, and calcium by at least 4 hours. May reduce efficacy of thyroid hormone replacement when co-administered.
Vitamin C high-dose pearls: Doses above 2 g/day increase oxalate excretion and should be avoided in patients with calcium oxalate nephrolithiasis history or severe renal impairment. Screen G6PD before IV ascorbate above 7.5 g.
Selenium: Toxic above 400 µg/day chronically. Selenosis presents with garlic breath, hair loss, brittle nails, and peripheral neuropathy. Do not exceed 200 µg/day in supplemental form, and account for dietary intake from Brazil nuts (which contain 70–90 µg per nut).
Pregnancy and lactation: NAC has been used in obstetric protocols for acetaminophen overdose and recurrent pregnancy loss with reasonable safety data. High-dose IV glutathione, the Milano cocktail, sulforaphane concentrates, and SAMe lack adequate pregnancy safety data and should be deferred. Methylation cofactors at standard prenatal doses are appropriate.
🌀
Differential Diagnosis: When Low Glutathione Is the Cause vs. a Consequence
Functional medicine literature often frames glutathione depletion as the upstream lesion, but in many clinical contexts low GSH is a downstream biomarker of an unaddressed primary process. Distinguishing these scenarios prevents indefinite supplementation that fails to resolve symptoms.
Primary glutathione synthesis defects are rare but real. Glutathione synthetase deficiency, glutamate-cysteine ligase deficiency, and 5-oxoprolinase deficiency are inborn errors presenting in childhood with hemolytic anemia, metabolic acidosis, and neurological symptoms. Adult-onset functional cysteine deficiency from chronic dietary inadequacy, malabsorption (post-bariatric surgery, celiac disease, inflammatory bowel disease), or methylation cycle blocks (severe B12, folate, or B6 deficiency) represents an acquired form. These patients respond directly to precursor supplementation.
Glutathione depletion as a consequence occurs in: active chronic infection (Epstein-Barr reactivation, chronic hepatitis B/C, HIV, tuberculosis, Lyme co-infections), uncontrolled diabetes with HbA1c above 8.5%, ongoing heavy metal exposure (occupational, dental amalgam in symptomatic individuals, contaminated water), persistent mold biotoxin exposure, untreated obstructive sleep apnea with nocturnal hypoxia, and chronic NSAID, acetaminophen, or alcohol use. In all of these, supplementing glutathione without removing the upstream driver yields transient biomarker improvement followed by regression.
Suggested differential algorithm: A patient with low erythrocyte GSH should undergo screening for chronic viral hepatitis (HBsAg, anti-HCV), HIV, HbA1c, ferritin and transferrin saturation (for hemochromatosis), heavy metal panel (whole blood mercury, lead, cadmium; provoked urinary metals are controversial and should be ordered cautiously), 25-OH vitamin D, and B12/folate/homocysteine. Sleep history, occupational history, and medication list complete the workup. If a primary driver is identified, it must be addressed before or in parallel with antioxidant support.
Red flags suggesting non-redox pathology: unintentional weight loss, night sweats, lymphadenopathy, persistent fevers, focal neurological signs, and biomarker shifts that do not improve despite full protocol adherence. These patients require oncologic and infectious disease evaluation rather than escalating supplement doses.
The redox framework is a powerful clinical tool, but it is a window into systemic biology, not a closed therapeutic loop. Restoring glutathione is necessary in many cases and sufficient in few.