The Silent Epidemic Living in Your Stomach
Helicobacter pylori is a gram-negative, spiral-shaped bacterium that has co-evolved with humans for at least 60,000 years. It colonizes the gastric mucosa of approximately 50% of the world population. H. pylori produces urease, an enzyme that converts urea into ammonia and carbon dioxide, effectively neutralizing the hydrochloric acid in its immediate environment.
How H. pylori Causes Disease: From Gastritis to Cancer
The clinical consequences follow the Correa cascade: chronic active gastritis progresses to atrophic gastritis, intestinal metaplasia, dysplasia, and ultimately gastric adenocarcinoma. The WHO classified H. pylori as a Group 1 carcinogen in 1994. It accounts for approximately 90% of duodenal ulcers and 75% of all stomach cancers worldwide.
The Growing Crisis of Antibiotic Resistance
Standard first-line triple therapy (PPI + clarithromycin + amoxicillin) eradication rates have fallen below 80% in most populations. Global clarithromycin resistance now ranges from 15% to over 40%. The Maastricht VI Consensus Report (2022) now recommends susceptibility-guided therapy wherever possible.
Furthermore, repeated courses of broad-spectrum antibiotics disrupt the gut microbiome, increasing the risk of C. difficile infection and long-term dysbiosis.
Evidence-Based Natural Treatment Protocol
1. Curcumin (Turmeric Extract)
Curcumin inhibits NF-kB signaling and has been shown to directly inhibit bacterial growth in vitro. A 2020 RCT showed that adding curcumin to triple therapy increased eradication rates from 72.6% to 88.9%. Protocol: 500-1000 mg curcumin twice daily with meals. Duration: 4-8 weeks.
2. Propolis (Bee Propolis Extract)
Boyanova et al. (2015) demonstrated bactericidal activity against H. pylori strains, including clarithromycin-resistant isolates. Protocol: 400-600 mg standardized propolis extract daily. Duration: 4-8 weeks.
3. Mastic Gum (Pistacia lentiscus)
Dabos et al. (2010) showed pure mastic gum at 350 mg three times daily eradicated H. pylori in nearly 30% of patients as monotherapy. Protocol: 350 mg three times daily on an empty stomach. Duration: 4-8 weeks.
4. Zinc Carnosine
Mahmood et al. (2007), publishing in Gut, demonstrated that zinc carnosine stabilizes gastric mucosa and accelerates ulcer healing. Protocol: 75 mg twice daily between meals. Duration: 8 weeks.
| Natural agent | Daily dose |
|---|---|
| Curcumin | 500-1000 mg twice daily |
| Propolis | 400-600 mg |
| Mastic gum | 350 mg three times daily |
| Zinc carnosine | 75 mg twice daily |
Restoring the Gastric Mucosa
L-Glutamine: 2-5 grams daily on an empty stomach supports mucosal repair. DGL (Deglycyrrhizinated Licorice): 380-760 mg chewable tablets before meals stimulates mucus production. Slippery Elm: 1-2 tablespoons in warm water between meals provides a protective coating.
Diagnostic Methods
Urea Breath Test (UBT): Sensitivity and specificity both exceed 95%. Preferred for initial diagnosis and confirming eradication. Stool Antigen Test: Sensitivity ~95%. Excellent alternative for pediatric patients. Endoscopic Biopsy: Mandatory when alarm symptoms are present.
Dietary Strategies
Broccoli Sprouts (Sulforaphane): Yanaka et al. (2009, Cancer Prevention Research) showed 70g daily for 8 weeks significantly reduced H. pylori colonization. Cabbage Juice: Rich in vitamin U (S-methylmethionine) that supports mucosal repair. Foods to Include: omega-3 fish, extra virgin olive oil, fermented vegetables, green tea, manuka honey, garlic, ginger. Foods to Avoid: spicy foods, alcohol, coffee on empty stomach, fried/processed meats.
When Antibiotics Are Absolutely Necessary
Active peptic ulcer disease, MALT lymphoma, atrophic gastritis with intestinal metaplasia, family history of gastric cancer, and prior to long-term NSAID therapy all require antibiotic-based eradication.
Frequently Asked Questions
Can H. pylori be completely eradicated naturally? In some cases, yes. Mastic gum monotherapy achieves ~30% eradication. Combining multiple agents may increase this rate. If infection persists after 8-12 weeks, antibiotics should be reconsidered.
How long does mucosal healing take? Superficial gastritis typically resolves within 4-8 weeks. Atrophic gastritis may take 6-12 months. Intestinal metaplasia rarely reverses completely.
Are probiotics helpful? Yes. Meta-analyses show probiotics improve eradication rates by 10-15% and reduce antibiotic side effects by 30-40%. Best strains: S. boulardii, L. rhamnosus GG.
Can H. pylori come back? Reinfection rates: 1-3% annually in developed countries, 10-15% in developing countries. Good hygiene and clean water reduce risk.
Is it safe to combine supplements with antibiotics? Most agents discussed are safe as adjuncts. Take DGL and slippery elm 2 hours apart from antibiotics to avoid absorption interference.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before starting any treatment protocol.
🌀
Confirming Eradication: Which Test, When, and Washout Rules
Symptom relief is not a surrogate for microbiological cure. Maastricht VI/Florence guidance and the American College of Gastroenterology recommend objective post-treatment testing in every patient treated for H. pylori, regardless of therapy used PMID: 28456631. Failure to confirm eradication leaves the Correa cascade active and exposes the patient to ongoing oncologic risk.
Two non-invasive assays are validated for test-of-cure: the urea breath test (13C-UBT) and the monoclonal stool antigen test. Both reach sensitivity above 90% and specificity above 95% when timing rules are respected PMID: 28071659. Serology must not be used for confirmation — IgG titres persist for months to years after bacterial clearance and cannot distinguish active from past infection.
The mandatory washout intervals are: at least four weeks after the last dose of any antibiotic or bismuth-containing compound, and at least two weeks after the last dose of a proton pump inhibitor. The same window applies to high-dose H2-blockers. Plant compounds with documented anti-urease activity (mastic gum, propolis, broccoli-sprout sulforaphane) have not been formally validated as causes of UBT false-negatives, but a conservative two-week pause before testing is reasonable given their mechanism.
Testing is performed no earlier than four weeks after completion of therapy. Earlier sampling captures suppressed but viable organisms and yields false-negative results that later relapse. If the patient required endoscopy for an independent indication (alarm symptoms, ulcer follow-up, intestinal metaplasia surveillance), histology plus rapid urease test from biopsies of both antrum and corpus is acceptable; corpus sampling is essential in patients still on PPI because acid suppression shifts colonisation proximally.
A negative confirmatory test does not close the file in patients with atrophic gastritis or intestinal metaplasia. These patients carry residual gastric cancer risk that persists after successful eradication and require endoscopic surveillance stratified by OLGA/OLGIM stage. Reinfection rates in adults from high-income regions remain below 2% per year; a previously negative patient who develops recurrent symptoms should still be retested rather than empirically retreated.
🌀
Contraindications, Interactions and Monitoring of the Herbal Protocol
The natural agents described carry a non-trivial safety profile that must be screened before initiation.
Curcumin at 1–2 g/day has low intrinsic toxicity but is a potent inhibitor of CYP3A4, CYP2C9 and P-glycoprotein. Clinically relevant interactions are documented with warfarin (INR elevation), direct oral anticoagulants, tacrolimus and several tyrosine kinase inhibitors. It should be paused 7–10 days before any elective procedure with bleeding risk. Curcumin also stimulates gallbladder contraction and is contraindicated in symptomatic cholelithiasis or biliary obstruction.
Mastic gum is generally well tolerated; the principal precaution is cross-reactivity in patients with Anacardiaceae or Pistacia allergy. No clinically significant cytochrome interactions are described, but the resin can cause mild epigastric burning at doses above 1 g/day.
Propolis at 400–600 mg/day is contraindicated in patients with bee-product allergy; anaphylaxis has been reported. It exhibits mild antiplatelet activity and should be reviewed in patients on dual antiplatelet therapy or anticoagulation.
Zinc carnosine at 75 mg twice daily delivers approximately 34 mg elemental zinc per day. Use beyond eight weeks at this dose may induce copper deficiency with secondary sideroblastic anaemia and neuropathy; serum copper and ceruloplasmin should be checked if therapy is extended.
DGL (deglycyrrhizinated licorice) by definition removes glycyrrhizin, but quality varies and adulterated products have caused pseudohyperaldosteronism with hypertension, hypokalaemia and oedema. Source verification matters; whole-licorice extracts must not be substituted.
Broccoli-sprout sulforaphane is contraindicated in patients on warfarin without INR monitoring because of competing vitamin K content in sprouts and in patients with overt hypothyroidism due to goitrogen load at sustained intake above 100 g/day.
Baseline workup before a 4–8 week protocol: CBC, comprehensive metabolic panel, INR if anticoagulated, and a medication reconciliation focused on CYP3A4 substrates. Re-check liver enzymes at week 4 in patients on curcumin plus other hepatically cleared drugs.
🌀
Probiotic Adjuvants: Strain-Level Evidence
Probiotics do not eradicate H. pylori as monotherapy. Their documented role is as adjuvants to antibiotic regimens, where they reduce therapy-associated diarrhoea and modestly improve eradication rates. Evidence is strain-specific and cannot be generalised across the "probiotic" category.
Saccharomyces boulardii CNCM I-745 at 500 mg twice daily, co-administered with triple or quadruple therapy for two weeks, is a well-studied adjuvant that modestly improves eradication rates and reduces antibiotic-associated diarrhoea. The yeast is contraindicated in central venous catheters and in severely immunocompromised patients because of rare fungaemia.
Lactobacillus reuteri DSM 17938 and ATCC PTA 6475 at 2×10^8 CFU twice daily showed adjuvant benefit in eradication and symptom scores when given alongside standard therapy PMID: 19298337. Effect size is smaller than S. boulardii in pooled analyses.
Multi-strain formulations containing Lactobacillus and Bifidobacterium have inconsistent results, with modest improvement in eradication rate reported when co-administered for at least 14 days. Duration shorter than two weeks does not produce a measurable effect.
Timing matters: probiotics should be taken at least two hours apart from antibiotic doses to limit direct killing. Continuation for two to four weeks after antibiotic completion supports microbiome recovery but does not further influence eradication. None of these agents replaces confirmatory testing.
🌀
When Natural Therapy Fails: Structured Salvage
If post-treatment UBT or stool antigen remains positive, the regimen has failed and the patient requires reconsideration of strategy rather than repetition of the same protocol.
First-line failure of any regimen — natural, triple or quadruple — should trigger a resistance-guided decision. Clarithromycin resistance rates above 15% in the local population invalidate empirical clarithromycin-containing triple therapy PMID: 28456631. Where culture and susceptibility testing are available (endoscopic biopsy with E-test), tailored therapy yields eradication rates above 90%. Where unavailable, regimen choice should rotate antibiotic classes.
Bismuth quadruple therapy (bismuth subcitrate or subsalicylate, PPI, tetracycline, metronidazole) for 14 days is the preferred empirical salvage and overcomes most clarithromycin and metronidazole resistance. Eradication rates of 85–95% are reported in resistant populations.
High-dose dual therapy with a potent acid suppressant (vonoprazan where licensed, or high-dose PPI such as esomeprazole 40 mg four times daily) plus amoxicillin 750 mg four times daily for 14 days is an alternative when bismuth is not tolerated; it preserves activity against clarithromycin- and metronidazole-resistant strains.
Levofloxacin-containing triple therapy is reserved for third-line use because of escalating fluoroquinolone resistance and tendinopathy risk. After two failed regimens, referral for endoscopy with culture is mandatory.
Throughout salvage, herbal adjuvants documented in earlier RCTs (curcumin, mastic gum, broccoli-sprout sulforaphane) may be continued alongside antibiotics; available data suggest additive benefit without pharmacokinetic interference. Confirmatory testing rules remain unchanged: minimum four-week post-antibiotic and two-week post-PPI washout.
🌀
Differential Diagnosis Before Attributing Symptoms to H. pylori
H. pylori positivity in a symptomatic patient does not establish causality. Up to half of carriers are asymptomatic, and dyspepsia has multiple non-bacterial causes that must be excluded before therapy is initiated or extended.
Functional dyspepsia (Rome IV) accounts for the majority of unexplained epigastric pain. It is diagnosed when alarm features are absent, organic pathology is excluded by endoscopy in patients above 50 or with red flags, and symptoms persist at least three months. Eradication of H. pylori in functional dyspepsia produces durable symptom relief in only a minority of cases (number needed to treat approximately 14).
Gastro-oesophageal reflux disease frequently overlaps with dyspeptic symptoms and is not improved — and may transiently worsen — after H. pylori eradication in patients with corpus-predominant gastritis.
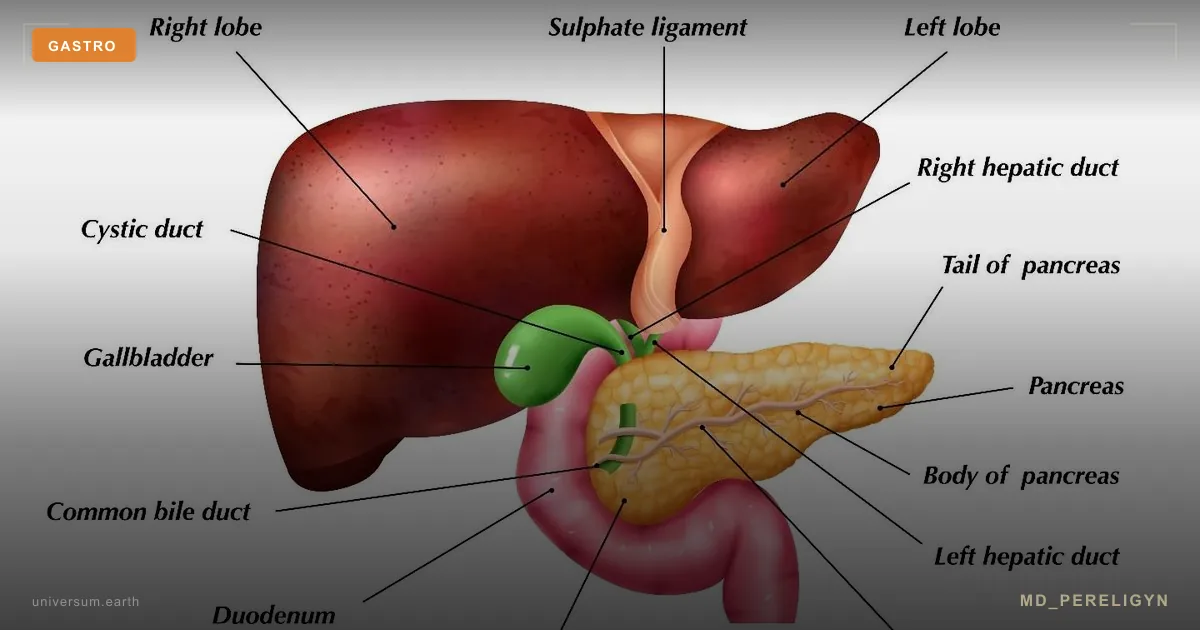
Biliary pathology (symptomatic cholelithiasis, sphincter of Oddi dysfunction) produces post-prandial right upper quadrant or epigastric pain often misattributed to gastritis. Right upper quadrant ultrasound is the first-line test when symptoms are post-prandial or fatty-food triggered.
Pancreatic disease, including chronic pancreatitis and pancreatic adenocarcinoma in patients over 50 with new-onset dyspepsia plus weight loss, requires cross-sectional imaging.
Cardiac ischaemia presenting as epigastric burning is the most consequential miss in patients with cardiovascular risk factors; an ECG is warranted in any patient over 40 with new epigastric pain plus exertional component or autonomic features.
Drug-induced gastropathy from NSAIDs, low-dose aspirin, bisphosphonates, iron salts and SSRIs is independent of H. pylori status. Medication review precedes both diagnostic testing and natural therapy. Alarm features — weight loss, dysphagia, anaemia, haematemesis, melaena, persistent vomiting, family history of gastric cancer in a first-degree relative under 50, or onset above 55 — mandate endoscopy before any empirical treatment.
References
- PMID: 28456631. PMID 28456631
- PMID: 28071659. PMID 28071659
- PMID: 19298337. PMID 19298337