Introduction: the endothelium as the largest endocrine organ
When people say “blood vessel,” they often imagine a pipe. It is a convenient metaphor, but physiologically it is wrong. The endothelium, the thin inner lining of the vessel, is an active endocrine organ with a total weight of about 1.5 kg and a surface area of approximately 4,000 square meters — larger than a standard football field.
This organ synthesizes nitric oxide (NO), prostacyclin, endothelin, thrombomodulin, and tissue plasminogen activator. It regulates vascular tone, coagulation, permeability, angiogenesis, and the immune response. When it functions properly, blood flow is laminar, blood pressure is stable, platelets do not aggregate, and monocytes do not adhere.
Key idea of the md_pereligyn protocol: endothelial dysfunction precedes visually detectable atherosclerotic plaque by 10–20 years. This is an intervention window in which functional reversibility has been demonstrated in peer-reviewed data.
In other words: the vessel begins to become diseased long before chest pain appears. If caught at this stage, atherosclerosis can be halted before it progresses to stenting, bypass surgery, or myocardial infarction.
🌀
What a healthy endothelium does
Six functions without which the vascular system collapses:
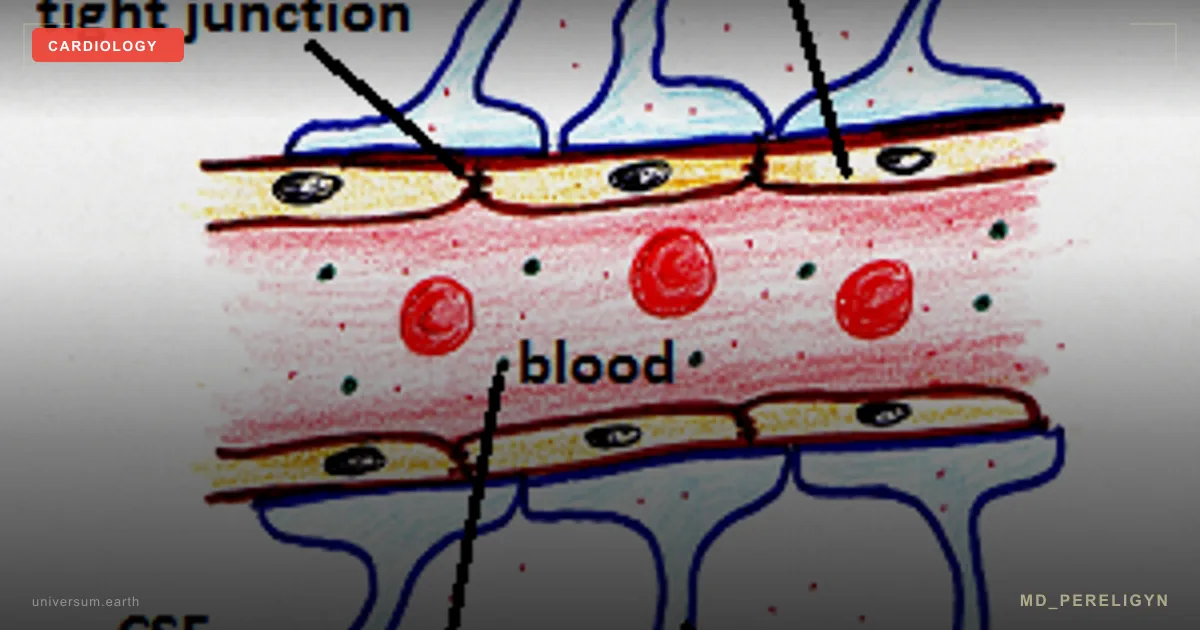
▸Vasodilation via NO — eNOS (endothelial NO synthase) converts L-arginine into NO; NO diffuses into smooth muscle, activates guanylate cyclase, and relaxes the vessel. ▸Antithrombotic effect — thrombomodulin activates protein C and blocks thrombin; heparan sulfates in the glycocalyx prevent platelet aggregation. ▸Barrier function — selective permeability and retention of albumin within the vascular bed. ▸Inflammation control — expression of adhesion molecules (VCAM-1, ICAM-1, E-selectin) is switched on only in response to an injury signal. ▸Fibrinolysis — release of tissue plasminogen activator (t-PA) to dissolve microthrombi. ▸Angiogenesis — synthesis of VEGF during ischemia and formation of collateral vessels.
All six functions require sufficient NO bioavailability. NO is the central molecule of endothelial health.
🌀
Mechanisms of dysfunction
Endothelial dysfunction is not “everything breaking at once,” but a cascade with a key fork: decreased NO + increased oxidative stress.
▸Oxidative stress reduces NO bioavailability. The superoxide anion (O2⁻) reacts with NO within nanoseconds, forming peroxynitrite (ONOO⁻). NO disappears, and peroxynitrite damages proteins and DNA. ▸ADMA — asymmetric dimethylarginine — is an endogenous inhibitor of eNOS. ADMA concentrations rise in CKD, diabetes, and hypertension. Each μmol/L increase in ADMA raises cardiovascular risk by 22% (Schnabel R, Circ Res 2005, PMID 16100045[1]). ▸Oxidized LDL penetrates the subendothelial space through the damaged glycocalyx and attracts monocytes. ▸Monocytes transform into macrophages, engulf oxidized LDL, and become foam cells — this is the core of the future plaque. ▸Smooth muscle migrates into the intima, produces collagen, and forms a fibrous cap.
After 10–20 years, the process becomes visually detectable on ultrasound or CT. But the first steps — reduced FMD (flow-mediated dilation) and increased ADMA — can be detected one and a half to two decades earlier.
🌀
Drivers of dysfunction
Eight factors, each of which independently increases the risk of dysfunction by 20–60%. In combination, the effect is multiplicative.
•Hyperglycemia — protein glycation (HbA1c, fructosamine), formation of AGE products, and oxidative stress. Even prediabetes with HbA1c 5.7–6.4% increases the risk of endothelial dysfunction by 40%. •Visceral fat — adipocytes in the visceral depot secrete TNF-α, IL-6, leptin, and resistin. This is systemic low-grade inflammation that keeps the endothelium activated. •Arterial hypertension — increased shear stress and elevated endothelin-1. The paradox: moderate shear stress activates eNOS; excessive shear stress causes injury. •Chronic stress — cortisol increases blood pressure, and sympathetic activation depletes NO through catecholamines. •Sleep under 6 hours — reduced parasympathetic activity, higher evening cortisol, and impaired glycocalyx recovery. •Smoking — nicotine reduces eNOS, and carbon monoxide displaces NO from myoglobin and hemoglobin. •Vitamin D deficiency (<30 ng/mL) — vitamin D regulates eNOS expression; deficiency is associated with increased ADMA. •Omega-3 deficiency — an omega-3 index <4% is accompanied by a twofold increase in the risk of endothelial dysfunction.
🌀
Markers of early dysfunction
When a standard cardiologist says, “cholesterol is normal, ECG is clean, go home,” early dysfunction remains unnoticed. What actually reflects endothelial status:
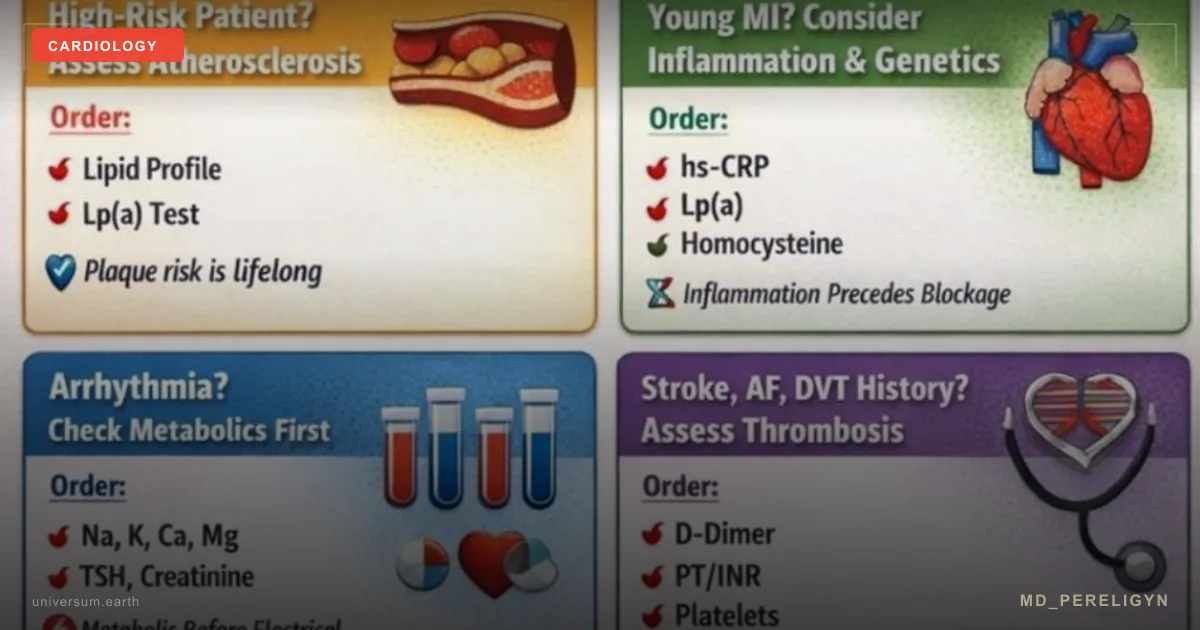
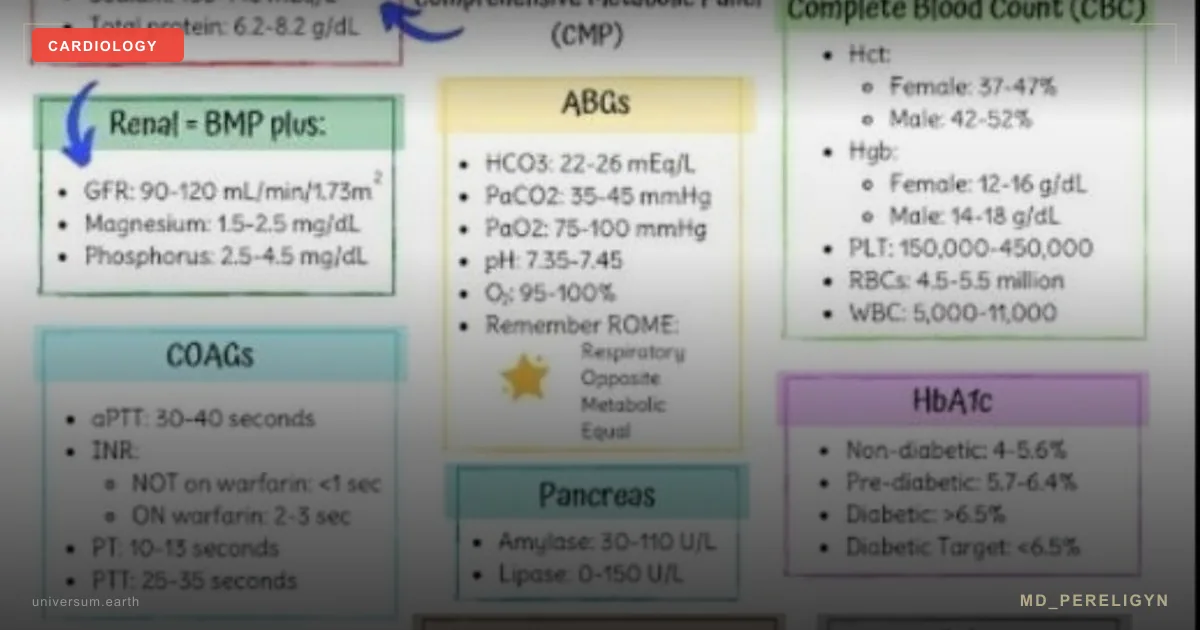
▸FMD (flow-mediated dilation) — the gold standard. Ultrasound of the brachial artery before and after 5-minute occlusion. Normal >7%, dysfunction <4%. ▸hsCRP — high-sensitivity C-reactive protein. Target <1 mg/L. >3 mg/L indicates high vascular risk. ▸ADMA / SDMA — direct markers of eNOS inhibition. Available in commercial laboratories (Germany, USA). ▸Omega-3 index — % EPA+DHA in erythrocyte membranes. Target >8%, risk zone <4%. ▸Small dense LDL (sdLDL) and oxLDL — atherogenic subfractions that penetrate the subendothelial space. ▸Microalbuminuria — an indicator of systemic endothelial dysfunction, detected years before diabetic nephropathy. ▸Lp(a) — an independent genetic factor of endothelial injury. Tested once. ▸ApoB / ApoA1 ratio — predicts risk better than total cholesterol.
| Marker | Target | Risk zone |
|---|---|---|
| FMD | > 7% | < 4% |
| hsCRP | < 1 mg/L | > 3 mg/L |
| Omega-3 index | > 8% | < 4% |
A detailed review of which tests to order first is in the article Early markers of cardiovascular risk (in preparation).
🌀
A holistic protocol for supporting the NO factory
The principle of the md_pereligyn protocol: treatment is directed not at the plaque, but at the vessel. Restoring endothelial function stops the progression of atherosclerosis years before surgery becomes necessary.
1. NO precursors
▸L-arginine 3–6 g/day — a substrate for eNOS. Take on an empty stomach, divided into 2–3 doses. ▸L-citrulline 3 g/day — bypasses first-pass arginase metabolism in the liver and raises plasma arginine more reliably than arginine itself. ▸Betaine (trimethylglycine) 1500 mg — lowers homocysteine; a cofactor for remethylation.
Caution: L-arginine is contraindicated in active HSV (the herpes virus uses arginine for replication); in oncologic disease with increased tumor perfusion, discuss with a physician.
2. Antioxidant protection
▸Vitamin C 500–1000 mg — regenerates tetrahydrobiopterin (BH4), an eNOS cofactor. ▸N-acetylcysteine (NAC) 600–1200 mg — a glutathione precursor. ▸Glutathione (liposomal) 250–500 mg or its precursors (glycine 3 g + cysteine 500 mg).
3. Polyphenols — BH4 regeneration
When BH4 is oxidized to BH2, eNOS becomes “uncoupled” and starts producing superoxide instead of NO. This is a critical point.
▸Pomegranate (extract) 250–500 mg — punicalagin, with a proven effect on FMD (Aviram M, Clin Nutr 2004, PMID 15158307[2]). ▸Cocoa (flavanols) 500 mg — epicatechin increases FMD by 3–5% within 2 hours. ▸Resveratrol 250–500 mg — SIRT1 activation and eNOS phosphorylation. ▸Quercetin 500 mg — blood pressure reduction and antioxidant effect. ▸Epigallocatechin-3-gallate (EGCG) 400 mg — green tea extract.
4. Omega-3
▸EPA+DHA 2 g/day (based on REDUCE-IT, target EPA is 4 g in high-risk patients). ▸Check the omega-3 index every 4–6 months; target >8%. ▸Quality is critical: fish oil must be tested for oxidation (TOTOX <26).
5. Magnesium and minerals
▸Magnesium (glycinate / taurate) 400 mg — an eNOS cofactor and direct vascular relaxant. ▸Potassium through diet — leafy greens, avocado, legumes. Target 4–5 g/day.
6. Vitamin D + K2
▸Vitamin D3 to a level of 60–80 ng/mL, with doses of 4,000–10,000 IU/day individualized. ▸Vitamin K2 (MK-7) 100–200 mcg — directs calcium into bones and teeth and protects against vascular calcification. Without K2, high doses of D3 increase the risk of arterial calcification.
7. Movement and shear stress
▸Aerobic exercise 30+ minutes/day — walking, swimming, cycling. Laminar shear stress activates eNOS. ▸Strength training 2–3 times/week — supports muscle mass and insulin sensitivity. ▸HIIT with caution — in patients with already reduced FMD, intense intervals may increase oxidative stress.
8. Nutrition
▸Mediterranean / DASH pattern — olive oil, fish, vegetables, nuts, legumes. ▸Limiting omega-6 — sunflower and corn oil, fast food. ▸Limiting fast carbohydrates and fructose — fructose directly damages the glycocalyx. ▸Nitrate-rich vegetables — beetroot, spinach, arugula: the dietary NO pathway via nitrate → nitrite → NO, independent of eNOS.
🌀
What does NOT work (and why)
▸Isolated cholesterol lowering with statins without lifestyle work — slows progression but does not restore FMD to youthful levels. ▸Aspirin “just in case” — in patients without clear risk, modern recommendations (USPSTF 2022) do not support primary prevention. Bleeding outweighs benefit. ▸Oxidized fish oil — TOTOX > 26 produces a pro-oxidant effect, the opposite of what is desired. ▸Isolated vitamin D without K2 at doses >5,000 IU for prolonged periods — risk of arterial calcification. ▸L-arginine in active HSV — feeds the virus and provokes flare-ups. ▸High-dose antioxidants as monotherapy (for example, beta-carotene in one study increased lung cancer risk in smokers) — polyphenol complexes are needed, not single nutrients in megadoses.
🌀
When to seek evaluation
▸Family history of coronary artery disease, myocardial infarction, or stroke before age 60 ▸CAC score > 0 before age 50 ▸Metabolic syndrome, prediabetes, type 2 diabetes ▸Visceral fat > 10 (DEXA) or waist circumference > 94 cm (men) / > 80 cm (women) ▸Persistent fatigue or reduced exercise tolerance without an obvious cause ▸hsCRP > 2 mg/L on repeated tests
I provide comprehensive vascular health screening (FMD, ADMA, an expanded lipid panel with sdLDL and Lp(a), omega-3 index) and create a personalized protocol to restore the NO factory.
🌀
Conclusion
The endothelium is therapeutic target No. 1 in the cardiology of the future. Not the plaque. Not cholesterol in isolation. Not a resting ECG. The functional state of the largest endocrine organ in the body.
Dysfunction begins 10–20 years before clinical symptoms. This is a unique window in which reversibility has been proven. A holistic protocol — NO precursors, antioxidants, polyphenols, omega-3, magnesium, vitamin D + K2, movement, and nutrition — restores NO bioavailability and halts the progression of atherosclerosis.
The vessel should be treated, not its complications.
🌀
Sources
▸Vita JA. Endothelial function. Circulation 2011;124:e906–e912. PMID 22184047 ▸Förstermann U, Xia N, Li H. Roles of vascular oxidative stress and nitric oxide in the pathogenesis of atherosclerosis. Eur Heart J 2017;38:64–73. PMID 27664942 ▸Dimmeler S, Zeiher AM. Endothelial cell apoptosis in angiogenesis and vessel regression. Circ Res 2000;87:434–439. PMID 10988233 ▸Bahadoran Z, Mirmiran P, Ghasemi A. Role of nitric oxide in insulin secretion and glucose metabolism. Trends Endocrinol Metab 2020;31:118–130. PMID 31690508 ▸Schnabel R, Blankenberg S, Lubos E, et al. Asymmetric dimethylarginine and the risk of cardiovascular events. Circ Res 2005;97:e53–e59. PMID 16100045 ▸Aviram M, et al. Pomegranate juice consumption reduces carotid intima-media thickness and LDL oxidation. Clin Nutr 2004;23:423–433. PMID 15158307
Related articles: Cholesterol without statins, Magnesium for blood vessels.
🌀
FAQ
Can the endothelium be restored after years of smoking and hypertension? Yes, partially. NO bioavailability begins to rise 4–8 weeks after smoking cessation and starting the protocol. Full functional recovery takes 6–12 months. FMD improves even in patients over 60 with consistent adherence.
Which lab tests should be ordered first? At minimum: hsCRP, omega-3 index, an extended lipid panel with sdLDL and Lp(a), HbA1c, fasting insulin, fasting glucose. When available — ADMA, brachial-artery FMD ultrasound, homocysteine. A complete panel and personalized interpretation are addressed during consultation.
Is long-term L-arginine supplementation safe? Yes, at 3–6 g/day for 6–12 months under monitoring. Contraindicated during active HSV (the herpes virus uses arginine for replication). In oncologic disease, only under physician supervision. Always start at low doses and titrate up.
Do I still need statins if I work on lifestyle? It depends on risk. With CAC > 100, LDL-C > 190 mg/dL, or familial hypercholesterolemia, statins are indicated regardless of lifestyle. At moderate risk, the endothelial restoration protocol may be the primary intervention. Decisions must be individualized with a physician.
How quickly can FMD improvement be expected? Acute effects of cocoa and pomegranate appear within 2 hours of intake (transient dilation). Chronic FMD improvement of 3–5% takes 8–12 weeks of consistent protocol. A stable plateau — 4–6 months. ADMA and the omega-3 index are monitored every 3 months.
This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.
References
- PMID 16100045. PMID 16100045
- PMID 15158307. PMID 15158307
- Vita JA. Endothelial function. Circulation 2011;124:e906–e912. PMID 22184047
- Förstermann U, Xia N, Li H. Roles of vascular oxidative stress and nitric oxide in the pathogenesis of atherosclerosis. Eur Heart J 2017;38:64–73. PMID 27664942
- Dimmeler S, Zeiher AM. Endothelial cell apoptosis in angiogenesis and vessel regression. Circ Res 2000;87:434–439. PMID 10988233
- Bahadoran Z, Mirmiran P, Ghasemi A. Role of nitric oxide in insulin secretion and glucose metabolism. Trends Endocrinol Metab 2020;31:118–130. PMID 31690508