Introduction: Why NAD+ Became the Symbol of Anti-Aging
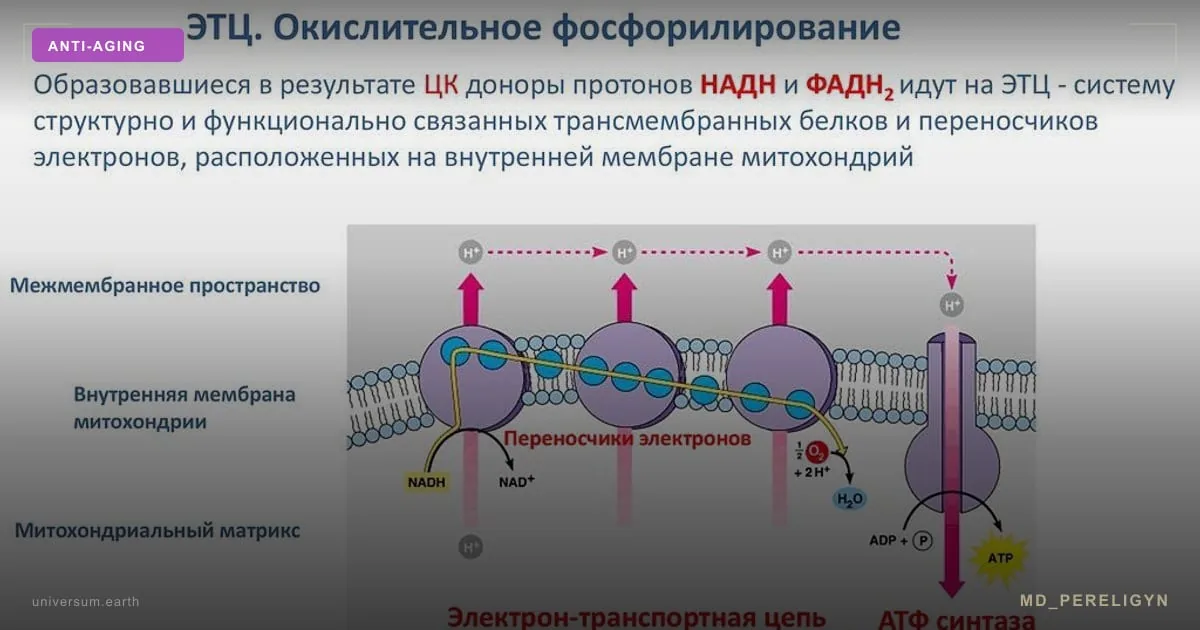
NAD+ (nicotinamide adenine dinucleotide) is a coenzyme present in every living cell. It participates in over 500 enzymatic reactions, including oxidative phosphorylation, DNA repair, and epigenome regulation. Massudi et al. (2012, PLoS ONE) demonstrated that human skin NAD+ levels decline by approximately 50% between ages 20 and 60.
This decline is associated with mitochondrial dysfunction, impaired DNA repair, chronic inflammation (inflammaging), and epigenetic drift — key hallmarks of aging described in the landmark paper by Lopez-Otin et al. in Cell (2013, updated 2023).
NAD+/NADH: Molecular Fundamentals
NAD+ exists in two forms: oxidized (NAD+) and reduced (NADH). The NAD+/NADH ratio is critical for metabolism: a high ratio (more NAD+) is associated with catabolism, fatty acid oxidation, and sirtuin activation. A low ratio (more NADH) signals anabolism and reduced cellular stress resilience.
NAD+ is synthesized through three pathways: de novo (from tryptophan), the salvage pathway (from nicotinamide via NAMPT), and the Preiss-Handler pathway (from nicotinic acid). The salvage pathway provides approximately 80% of cellular NAD+ and is the primary therapeutic target.
Sirtuins (SIRT1-7): Guardians of the Genome
Sirtuins are a family of NAD+-dependent deacetylases that play key roles in aging regulation. SIRT1 deacetylates histones and transcription factors (p53, FOXO, NF-kB), suppressing inflammation and activating DNA repair. SIRT3 is a mitochondrial sirtuin regulating beta-oxidation and antioxidant defense through SOD2.
A study in Nature (2013) showed that increasing SIRT1 activity in mice extends healthspan and improves metabolic parameters. SIRT6 is involved in telomere homeostasis, and its deficiency causes premature aging. All sirtuins are absolutely dependent on NAD+ — without it, their activity is impossible.
NMN vs NR: Which to Choose?
NMN (nicotinamide mononucleotide) is a direct NAD+ precursor requiring one enzymatic step for conversion (via NMNAT). Yoshino et al. (2021, Science) demonstrated that 250 mg NMN daily for 10 weeks raises blood NAD+ by 50% and improves insulin sensitivity in skeletal muscles of prediabetic women.
NR (nicotinamide riboside) is also a NAD+ precursor but requires two enzymatic steps (NRK to NMN to NAD+). Martens et al. (2018, Nature Communications) showed that 1000 mg NR (NIAGEN) daily for 6 weeks increases NAD+ by 60% in healthy older adults.
Comparison: - NMN: 250-500 mg/day, rapid conversion, good storage stability - NR: 300-1000 mg/day, longer research history, patented (NIAGEN) - Both forms effectively raise NAD+; no clinical superiority of one over the other has been established
| Form | Dose | Note |
|---|---|---|
| NMN | 250–500 mg/day | rapid conversion |
| NR | 300–1000 mg/day | patented (NIAGEN) |
IV NAD+ and NAD+ Biopellets: Advanced Methods
Intravenous NAD+ infusion (250-750 mg over 2-4 hours) provides 100% bioavailability, bypassing the GI tract. Clinical observations report rapid improvement in energy and cognitive function, but large RCTs are lacking. Common side effects include nausea, chest discomfort, and flushing during infusion.
NAD+ biopellets (subcutaneous pellets) are implantable capsules with slow NAD+ release, providing stable levels over several months. The method is evolving but lacks large-scale clinical data.
Epigenetic Clocks and NAD+
Epigenetic clocks (Horvath clock, GrimAge, DunedinPACE) measure biological age through DNA methylation patterns. A study in Aging Cell (2022) showed that raising NAD+ through NMN supplementation is associated with slower epigenetic aging, though large-scale RCTs using epigenetic clocks as a primary endpoint are pending.
David Sinclair at Harvard is the most prominent NAD+ and aging researcher. His lab demonstrated in Nature (2013) that boosting NAD+ through NMN reverses age-related mitochondrial decline in mice. However, translating results from mouse models to humans requires caution.
Other Strategies to Boost NAD+
Exercise is the most powerful natural NAD+ stimulator through AMPK activation and increased NAMPT expression. A study in Cell Metabolism (2019) showed a 127% increase in skeletal muscle NAD+ after 12 weeks of aerobic training.
Caloric restriction / intermittent fasting activates AMPK, which boosts NAMPT and increases NAD+ via the salvage pathway.
Niacinamide (vitamin B3) is a budget-friendly NAD+ precursor via the salvage pathway. Dose: 500-1000 mg/day. A study in Nature Aging (2022) showed a 40% NAD+ increase at 1000 mg/day.
NAD+ Therapy Protocol
Basic protocol: - NMN: 250-500 mg in the morning on empty stomach (sublingual or oral) - Or NR: 300-500 mg in the morning - Resveratrol: 500 mg with fatty food (SIRT1 activator) - TMG (trimethylglycine): 500 mg (methyl group compensation)
Advanced protocol (under medical supervision): - IV NAD+: 250 mg once every 2-4 weeks - NMN: 500 mg/day orally between infusions - Monitoring: blood NAD+ levels, epigenetic clocks every 6 months
Frequently Asked Questions
When should I expect results from NMN/NR? Subjective energy improvement: 2-4 weeks. Biomarker changes: 6-12 weeks. Epigenetic age effects: 6-12 months.
Is there a risk of cancer stimulation? Theoretical concern exists: cancer cells also need NAD+. A study in Nature Cell Biology (2019) showed NMN does not stimulate tumor growth in mice. Nevertheless, NAD+ therapy is contraindicated in active cancer.
Can NAD+ be raised through diet and exercise alone? Yes, exercise and fasting are powerful stimulators. However, after age 40-50, declining NAMPT makes supplementation justified.
What is the difference between NAD+ and NADH supplements? NADH is the reduced form. For anti-aging, it is important to raise NAD+ (the oxidized form), which activates sirtuins. NADH supplements are less effective for this purpose.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before starting any treatment protocol.
🌀
🌀
🌀
🌀