Introduction: the heart as an endocrine organ
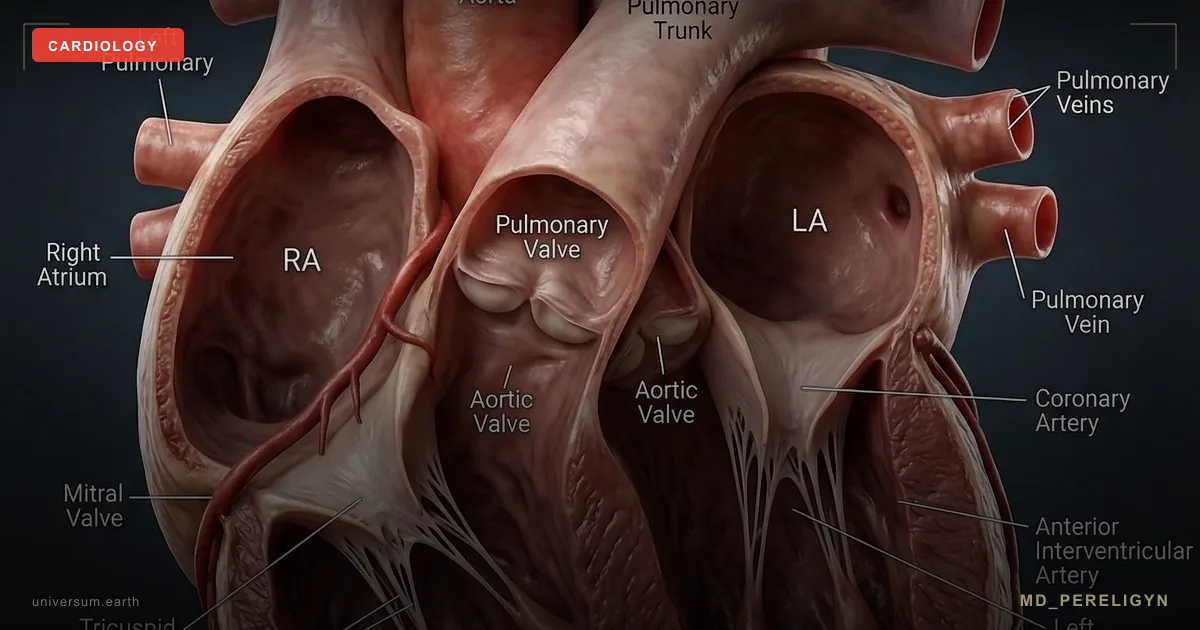
In the classical model, the heart is a pump: four chambers, valves, myocardium, and the conduction system. This model works for mechanics, but it is physiologically incomplete. Since 1981, it has been known that the heart is a fully functional endocrine organ that synthesizes its own family of hormones.
In 1981, de Bold and colleagues found that injection of atrial extract caused potent diuresis and natriuresis in rats (de Bold AJ, Life Sci 1981, PMID 7219045[1]). This discovery changed the understanding of cardiovascular regulation: the heart itself synthesizes a diuretic and vasodilator, antagonizing the renin-angiotensin-aldosterone system (RAAS).
Key idea of the md_pereligyn protocol: natriuretic peptides are an endogenous pharmacopoeia that works 24/7 without tablets. Their concentration and receptor sensitivity are modifiable parameters. NT-proBNP in a routine laboratory is a window into this system.
Understanding the peptide factory shifts cardiology from “pump repair” to “endocrine regulation.”
🌀
The natriuretic peptide family
Three key peptides:
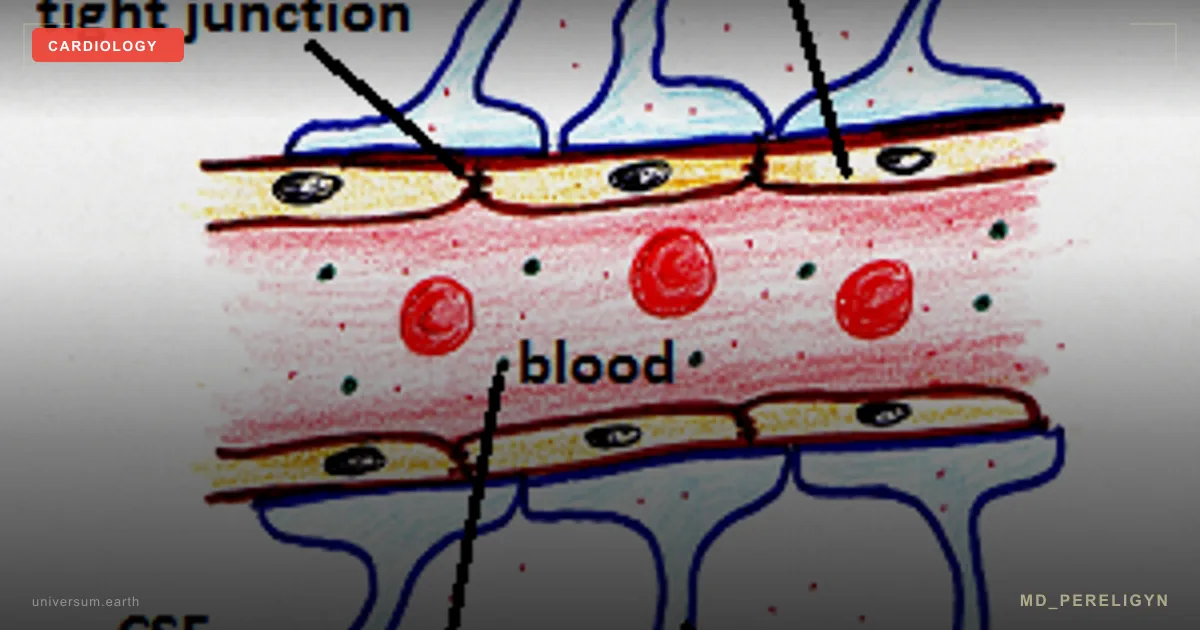
▸ANP (atrial natriuretic peptide) — synthesized by atrial cardiomyocytes in response to wall stretch. Its action is acute, over minutes. It stimulates diuresis, natriuresis, and vasodilation. ▸BNP (brain natriuretic peptide) — despite its name, because it was first isolated from porcine brain, its main source is the cardiac ventricles. Synthesis increases with ventricular overload. Its action is longer-lasting. ▸CNP (C-type natriuretic peptide) — produced by the endothelium and chondrocytes. It is a local paracrine regulator of vascular tone and bone growth.
All three act through NPR-A and NPR-B receptors, activating guanylate cyclase and increasing intracellular cGMP. The final effects are vasodilation and natriuresis.
Peptide degradation occurs through neutral endopeptidase (neprilysin) and the NPR-C clearance receptor. Modern ARNI-class drugs (sacubitril/valsartan) inhibit neprilysin, extending the life of the patient’s own peptides (McMurray JJV, NEJM 2014, PMID 25176015[2]).
🌀
Physiology of action
Natriuretic peptides are RAAS antagonists. They work in the opposite direction to angiotensin II and aldosterone.
▸Natriuresis — increased sodium excretion in the distal tubules through inhibition of reabsorption. ▸Diuresis — increased urine volume through suppression of ADH and direct tubular effects. ▸Vasodilation — relaxation of arteriolar smooth muscle via cGMP. ▸RAAS suppression — reduced renin and aldosterone secretion. ▸Sympathetic suppression — reduced central sympathetic activity. ▸Antifibrotic effect — suppression of myocardial myofibroblast proliferation. ▸Lipolysis — stimulation of visceral fat breakdown through the NPR-A receptor on adipocytes. In lean patients, BNP levels are higher than in patients with obesity under comparable hemodynamic load.
The obesity paradox: in obesity, NT-proBNP is underestimated by 30–50% relative to the true cardiac load. This masks early heart failure and requires BMI adjustment during interpretation.
🌀
When the heart increases synthesis
Stimuli that increase ANP/BNP synthesis:
•Wall stretch — the main trigger. Volume overload (hypervolemia, valvular regurgitation) or pressure overload (hypertension, aortic stenosis). •Heart failure — sustained NT-proBNP elevation is a diagnostic marker. •Acute ischemia — myocardial infarction increases BNP within 24–48 hours. •Arrhythmias — atrial fibrillation and tachycardia increase ANP. •Hypoxia — sleep apnea, COPD, pulmonary hypertension. •Acute physical exercise — a short-term physiological rise. •Pregnancy — physiological increase in the third trimester.
Stimuli that reduce synthesis or bioavailability:
•Obesity — increased clearance via NPR-C on adipocytes. •Young age and male sex — lower basal levels. •High-dose glucocorticoids — suppression of synthesis.
🌀
Biomarkers and diagnostic windows
Two main biomarkers are available in clinical practice:
▸NT-proBNP — the N-terminal fragment of proBNP. Half-life 60–120 min. Stable during collection and storage. Target ranges: • <125 pg/mL (age <75 years) — heart failure is unlikely • 125–450 pg/mL — gray zone, requires clinical interpretation • >450 pg/mL (<50 years), >900 (50–75), >1800 (>75) — high probability of HF ▸BNP — the biologically active peptide. Half-life 20 min. Less stable during storage. Target <100 pg/mL; >400 pg/mL — high probability of HF.
| NT-proBNP | Interpretation |
|---|---|
| <125 pg/mL | HF unlikely |
| 125–450 pg/mL | gray zone |
| >450 pg/mL | high probability of HF |
Other biomarkers:
▸MR-proANP (mid-regional proANP) — a stable proANP fragment. An alternative to NT-proBNP. ▸hsTnT / hsTnI (high-sensitivity troponin) — a marker of myocardial microinjury. Combined with NT-proBNP, it provides a more complete picture. ▸ST2 (soluble suppression of tumorigenicity 2) — a marker of fibrosis and remodeling. Prognostically independent of NT-proBNP. ▸Galectin-3 — myocardial fibrosis. A prognostic marker in chronic heart failure.
When to order NT-proBNP:
▸Dyspnea of unclear origin, to differentiate cardiogenic from pulmonary causes ▸Lower-extremity edema ▸Fatigue and reduced exercise tolerance ▸Hypertension with suspected occult HF ▸Screening in metabolic syndrome and type 2 diabetes ▸Before major surgery to assess cardiovascular risk ▸Monitoring chronic HF therapy — NT-proBNP reduction correlates with prognosis
🌀
Holistic protocol for supporting the peptide factory
Principle of the md_pereligyn protocol: the natriuretic system is a modifiable resource. Holistic work supports synthesis, receptor sensitivity, and clearance.
1. Reduction of visceral obesity
▸Weight loss of 5–10% — increases basal BNP and improves NPR-A receptor sensitivity. ▸Mediterranean / DASH pattern — olive oil, fish, vegetables, legumes. Reduction of visceral fat stores. ▸Strength training 2–3 times/week — support of muscle mass and metabolic flexibility. ▸Intermittent fasting 14:10 / 16:8 — improvement in HOMA-IR and reduction in fat mass.
2. Control of arterial hypertension
▸Target BP <130/80 — reduces chronic myocardial overload and stabilizes BNP within the physiological range. ▸Full hypertension protocol — see the BP article. ▸Addressing sleep apnea — nocturnal hypoxia and BP surges load the atria and ventricles.
3. Aerobic exercise
▸Walking 7–10 thousand steps/day — sustained physiological stimulation of BNP synthesis and increased receptor sensitivity. ▸Aerobic activity 30+ minutes/day — swimming, cycling. Acute BNP rise during exercise and resting adaptation. ▸HIIT 1–2 times/week — in cardiovascularly stable patients, improves VO2max and myocardial remodeling.
4. Omega-3 EPA+DHA
▸EPA+DHA 2 g/day — reduction of pressure overload, antifibrotic effect, and support of cardiomyocyte membranes. ▸Check the omega-3 index every 4–6 months, target >8%. ▸Quality is critical: fish oil should be tested for oxidation (TOTOX <26).
5. Magnesium and taurine
▸Magnesium (glycinate / taurate) 400 mg/day — a cofactor for cGMP synthesis and a direct vascular relaxant. ▸Taurine 1–3 g/day — modulation of cardiomyocyte calcium homeostasis and cardioprotection in chronic HF. ▸Potassium 4–5 g/day through diet — leafy greens, avocado, legumes.
6. CoQ10 and mitochondrial support
▸Ubiquinol (CoQ10) 100–200 mg/day — a cofactor for myocardial oxidative phosphorylation. In patients with chronic HF, it reduces mortality (Mortensen SA, JACC Heart Fail 2014, PMID 25282031[3]). ▸L-carnitine 1–2 g/day — transport of fatty acids into mitochondria. ▸D-ribose 5–10 g/day — a substrate for ATP synthesis when ejection fraction is reduced.
7. Vitamin D and K2
▸Vitamin D3 to a level of 50–80 ng/mL, with doses of 2,000–5,000 IU/day individualized. ▸Vitamin K2 (MK-7) 100–200 mcg — directs calcium into bone and protects against valve and vascular calcification.
8. Sleep and parasympathetic tone
▸Sleep 7–9 hours — a window for hormonal recovery and restoration of receptor sensitivity. ▸Breathing practices 10–20 min/day — slow diaphragmatic breathing (6 cycles/min) reduces preload. ▸HRV biofeedback — increase in parasympathetic tone.
🌀
What does NOT work
▸Ignoring NT-proBNP in obesity — underestimation by 30–50%. BMI adjustment is mandatory. ▸Isolated diuretic use without addressing the cause — reduces preload but does not solve the root cause of HF. ▸Chronic high-dose NSAID use — inhibits prostaglandins, increases sodium retention, and antagonizes peptides. ▸Chronic sleep deprivation and stress — increase sympathetic tone and RAAS activity, antagonizing the peptide system. ▸Isolated CoQ10 use without correcting hypertension and obesity — fragmented effect. ▸Self-discontinuation of ARNI / ACE inhibitors in chronic HF — abrupt withdrawal can cause decompensation.
🌀
When to seek care
▸Dyspnea with minimal exertion or at rest ▸Lower-extremity edema, especially in the evening ▸Nocturnal cough, orthopnea (needing to sit upright to breathe) ▸Fatigue and abrupt reduction in exercise tolerance ▸NT-proBNP >125 pg/mL (or above age-adjusted thresholds) ▸Previous myocardial infarction or atrial fibrillation ▸Family history of chronic HF or sudden cardiac death ▸Type 2 diabetes duration >10 years — screening for occult HF
I perform comprehensive cardiovascular screening (NT-proBNP, hsTnT, echocardiography with functional assessment, extended metabolic profile) and create a personalized protocol to support the natriuretic system.
🌀
Conclusion
The heart is an endocrine organ. Atrial and ventricular cardiomyocytes synthesize the natriuretic peptides ANP and BNP, the body’s own diuretic and vasodilator that antagonizes RAAS. This is an endogenous pharmacopoeia working 24/7.
NT-proBNP in a routine laboratory is a window into this system. A target level <125 pg/mL (with age adjustment) indicates preserved function. Elevation is an early signal of occult heart failure long before clinical symptoms appear.
The holistic protocol — reduction of visceral obesity, BP control, aerobic exercise, omega-3, magnesium, taurine, CoQ10, vitamin D + K2, and sleep — supports synthesis and receptor sensitivity. ARNI-class drugs extend the life of the patient’s own peptides, illustrating how modern pharmacology copies endogenous physiology.
Treatment should target regulation, not only symptoms.
🌀
Sources
▸de Bold AJ, Borenstein HB, Veress AT, Sonnenberg H. A rapid and potent natriuretic response to intravenous injection of atrial myocardial extract in rats. Life Sci 1981;28:89–94. PMID 7219045 ▸Levin ER, Gardner DG, Samson WK. Natriuretic peptides. NEJM 1998;339:321–328. PMID 9682046 ▸McMurray JJV, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. NEJM 2014;371:993–1004. PMID 25176015 ▸Mortensen SA, Rosenfeldt F, Kumar A, et al. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: results from Q-SYMBIO. JACC Heart Fail 2014;2:641–649. PMID 25282031 ▸Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2016;37:2129–2200. PMID 27206819 ▸Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J Am Coll Cardiol 2022;79:e263–e421. PMID 35379503
Related articles: Endothelium: foundation of vascular health, Cholesterol without statins.
🌀
FAQ
What does NT-proBNP show in practice? NT-proBNP is the most sensitive laboratory marker of heart failure. A level <125 pg/mL (age <75 years) makes HF unlikely, with high negative predictive value. Exceeding age-adjusted thresholds requires echocardiography and assessment of cardiac structure. The marker is also used to monitor therapy — a reduction in NT-proBNP during treatment is associated with improved prognosis.
Why can NT-proBNP be normal in a patient with obesity despite obvious HF? Adipocytes express NPR-C clearance receptors, which accelerate peptide removal from the blood. In patients with BMI >35, NT-proBNP is underestimated by 30–50% relative to the true cardiac load. Interpretation uses BMI adjustment or additional markers (MR-proANP, echocardiography).
Can endogenous natriuretic peptides be “boosted” without drugs? Yes, partially. Aerobic exercise, reduction of visceral fat, omega-3, magnesium, taurine, and BP control improve receptor sensitivity and support synthesis. ARNI drugs (sacubitril/valsartan) inhibit peptide degradation and prolong their half-life — they act on a molecule the body already synthesizes.
When should a healthy person order NT-proBNP? In dyspnea of unclear origin, edema, occult HF in the setting of diabetes or hypertension, before major surgery, or with a family history of chronic HF before age 60. Routine screening is not indicated in a young healthy person without symptoms. In metabolic syndrome or type 2 diabetes lasting >10 years, it is justified.
What is the difference between ARNI and a standard ARB? ARNI (sacubitril/valsartan) combines a neprilysin inhibitor, which increases levels of endogenous natriuretic peptides, with an ARB, which blocks angiotensin II. In PARADIGM-HF, cardiovascular death was reduced by 20% versus enalapril (McMurray 2014, PMID 25176015[2]). This is an example of targeted amplification of an endogenous system rather than replacement of it.
This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.
🌀
Interpreting borderline NT-proBNP: the 125–450 pg/mL grey zone
The article cites NT-proBNP <125 pg/mL as the rule-out threshold for chronic heart failure, but the 125–450 pg/mL range generates most clinical uncertainty. Age-stratified cut-offs refine interpretation. The ICON (International Collaborative of NT-proBNP) study established age-specific rule-in thresholds of 450 pg/mL (<50 years), 900 pg/mL (50–75 years), and 1800 pg/mL (>75 years) for acute heart failure, with a uniform rule-out value of 300 pg/mL in the acute setting. For chronic ambulatory diagnosis, the 125 pg/mL cut-off retains a negative predictive value above 94%, but specificity falls below 50% in patients over 75.
Three modifiers shift interpretation within the grey zone. First, renal function: NT-proBNP is cleared predominantly by the kidneys, and eGFR below 60 mL/min/1.73 m² raises the rule-in threshold by approximately 1.5–2-fold. A patient with eGFR 45 and NT-proBNP 300 pg/mL is more likely to have CKD-driven elevation than incident heart failure. Second, body mass index: adipocyte NPR-C receptors increase clearance, and patients with BMI >35 may have NT-proBNP values 30–50% lower for the same degree of cardiac stress PMID: 25176015. A value of 200 pg/mL in a patient with BMI 38 carries weight equivalent to 400 pg/mL in a lean patient. Third, atrial fibrillation: AF independently elevates NT-proBNP by a factor of 2–3 even in the absence of structural heart disease, and the rule-in threshold should be approximately doubled.
The practical algorithm in the 125–450 pg/mL range:
1. Repeat the test in 2–4 weeks under stable conditions (no recent illness, no recent exercise within 24 hours, no recent intravenous fluids). 2. If symptoms persist, obtain transthoracic echocardiography to assess left ventricular ejection fraction, diastolic function (E/e' ratio, left atrial volume index), and right ventricular function. 3. Add a high-sensitivity troponin to detect concurrent subclinical myocardial injury, which raises the pretest probability of HFpEF. 4. If echocardiography is normal but NT-proBNP remains elevated, consider non-cardiac causes (see next section).
The H2FPEF and HFA-PEFF scores incorporate NT-proBNP into a probability framework for HFpEF and outperform any single biomarker threshold PMID: 30025575. Neither replaces clinical judgement, but both reduce overdiagnosis in obese, hypertensive, and older patients where NT-proBNP carries reduced specificity.
🌀
Non-cardiac causes of elevated natriuretic peptides
NT-proBNP elevation is not synonymous with heart failure. The article frames the peptide as a "cardiac early warning," which is accurate but incomplete. Recognising non-cardiac elevations prevents unnecessary cardiology referrals and missed primary diagnoses.
Renal dysfunction is the single most common confounder. NT-proBNP rises in inverse proportion to eGFR, and patients on dialysis routinely have values above 1000 pg/mL without active cardiac decompensation. Pulmonary causes — acute pulmonary embolism, pulmonary hypertension of any aetiology, and severe pneumonia with right ventricular strain — elevate NT-proBNP through right-sided wall stress. In acute PE, NT-proBNP >600 pg/mL identifies intermediate-risk patients and influences thrombolysis decisions PMID: 24076282.
Sepsis elevates NT-proBNP through a combination of myocardial depression, fluid shifts, and inflammatory cytokine-mediated synthesis. Values often exceed 1000 pg/mL in septic patients without prior cardiac disease and normalise with resolution. Critical illness more broadly, including burns and major surgery, produces transient elevations.
Endocrine causes the article does not address include hyperthyroidism, which raises NT-proBNP through increased cardiac output and chronotropic stress, and Cushing's syndrome with secondary hypertension. Anaemia (haemoglobin below 100 g/L) elevates NT-proBNP through high-output physiology. Liver cirrhosis with portal hypertension produces cirrhotic cardiomyopathy and chronic NT-proBNP elevation independent of overt heart failure.
Drug-induced elevations include anthracycline chemotherapy (doxorubicin), trastuzumab, immune checkpoint inhibitors, and tyrosine kinase inhibitors. Serial NT-proBNP monitoring is now incorporated into cardio-oncology surveillance protocols. Recent intense exercise — particularly endurance events — produces transient elevations lasting 24–72 hours that resolve without intervention.
The clinical implication: an isolated elevated NT-proBNP without clinical context is uninterpretable. The minimum dataset before referral or treatment escalation includes creatinine and eGFR, complete blood count, TSH, liver function tests, and a directed history of recent illness, exercise, and medication exposure.
🌀
Exercise prescription stratified by ejection fraction
The article recommends 30 minutes of aerobic activity and HIIT 1–2 times per week without distinguishing between phenotypes of heart failure or preclinical risk. The evidence base supports differentiated prescriptions.
For patients with preserved cardiac function and isolated risk factors (hypertension, visceral obesity, NT-proBNP in the grey zone with normal echocardiogram), the prescription mirrors general cardiovascular prevention: 150 minutes per week of moderate-intensity continuous training at 60–70% of heart rate reserve, plus two sessions per week of resistance training. High-intensity interval training (4 × 4 minutes at 85–95% peak heart rate, separated by 3-minute recovery intervals) produces approximately 15% greater improvement in peak VO₂ compared to moderate continuous training in this population PMID: 27206819.
For patients with HFrEF (ejection fraction below 40%), the HF-ACTION trial established that supervised aerobic exercise reduces all-cause mortality or hospitalisation by 11% after adjustment for prognostic predictors, with no increase in adverse events. The protocol used 36 supervised sessions of treadmill or cycle ergometry at 60–70% of heart rate reserve, transitioning to 5 home sessions per week of 40 minutes at 60–70% intensity. Resistance training is permitted at 50–60% of one-repetition maximum, avoiding the Valsalva manoeuvre.
For HFpEF, the OptimEx-Clin and Ex-DHF trials showed that 12 weeks of HIIT or moderate continuous training improved peak VO₂ by approximately 1.5 mL/kg/min, although the effect on diastolic function was modest. HIIT is not superior to moderate continuous training in HFpEF, and adherence is higher with the latter.
Safety thresholds before initiating exercise:
- Systolic blood pressure should be below 180 mmHg and above 90 mmHg at rest. - Resting heart rate should be below 100 bpm. - NT-proBNP should be stable on serial measurement, not actively rising. - No exertional syncope, recent ventricular arrhythmia, or unstable angina within the prior six weeks.
Warning signs to stop a session and seek evaluation: chest pain or pressure not relieved by rest, orthopnoea developing during sleep on training days, weight gain greater than 2 kg over three days, or new resting heart rate above 100 bpm. Patients with implanted devices should avoid heart rates within 10 bpm of their ICD detection zone.
🌀
Supplement safety, interactions, and monitoring
The article recommends omega-3, magnesium, taurine, CoQ10, vitamin D, and vitamin K2 without addressing contraindications, drug interactions, or monitoring parameters. Each requires clinical framing before prescription.
Omega-3 EPA+DHA at 2 g/day prolongs bleeding time modestly and may interact with anticoagulants (warfarin, direct oral anticoagulants) and antiplatelets. At doses above 3 g/day, INR monitoring is appropriate for warfarin-treated patients, and bleeding events increase slightly in anticoagulated cohorts. Atrial fibrillation incidence increased modestly in REDUCE-IT and STRENGTH at icosapent ethyl doses of 4 g/day, an effect not consistently seen at 2 g/day mixed EPA+DHA. Patients with active bleeding, scheduled surgery within two weeks, or known fish allergy should not be prescribed high-dose omega-3.
CoQ10 (ubiquinol) at 100–200 mg/day reduces warfarin efficacy through structural similarity to vitamin K and can lower INR by 10–25%. Patients on warfarin require INR rechecking 1–2 weeks after initiation. CoQ10 modestly reduces systolic blood pressure (3–5 mmHg) and may potentiate antihypertensive therapy. The Q-SYMBIO trial supported its use in HFrEF as adjunct therapy with reduced major adverse cardiovascular events, but the trial used 300 mg/day in three divided doses.
Magnesium at 400 mg/day is well tolerated in patients with normal renal function but accumulates in CKD stage 3b or worse (eGFR <45 mL/min/1.73 m²). Hypermagnesaemia produces bradycardia, hypotension, and at serum levels above 2.5 mmol/L, neuromuscular paralysis. Magnesium also reduces absorption of bisphosphonates, tetracyclines, and levothyroxine — these should be spaced by four hours.
Vitamin K2 (MK-7) at 100–200 mcg directly antagonises warfarin and is contraindicated in patients on vitamin K antagonists. It does not interact with direct oral anticoagulants. Vitamin D3 at doses producing serum 25-OH-D above 80 ng/mL (200 nmol/L) carries a small risk of hypercalcaemia, particularly with concurrent calcium supplementation or thiazide diuretics. Serum calcium and 25-OH-D should be checked at three months after initiation, with annual monitoring thereafter.
Taurine at 1–3 g/day has the strongest safety record but is best avoided in patients with bipolar disorder due to anecdotal reports of mood destabilisation, and in those with severe hepatic impairment. None of these supplements should be initiated within 48 hours of cardiac surgery without surgical team approval, given bleeding and electrolyte considerations.
🌀
Serial monitoring and biomarker-guided therapy
Single NT-proBNP measurements have limited value beyond initial diagnosis. Serial measurement under stable conditions provides clinically actionable information. Intra-individual biological variation of NT-proBNP is approximately 30%, meaning a change of less than 30% between consecutive measurements may represent noise rather than disease evolution PMID: 35379503. A clinically meaningful change requires at least a 30% increase or decrease, and ideally a 50% change to confidently attribute it to treatment response or disease progression.
For asymptomatic patients with grey-zone values (125–450 pg/mL), recheck at 6–12 months under standardised conditions: morning sample, fasting state, no exercise within 24 hours, no acute illness within two weeks. For patients on HFrEF guideline-directed medical therapy, NT-proBNP should be measured at baseline and 3 months after each dose titration. A failure to decline by at least 30% from baseline despite optimisation warrants escalation to ARNI or specialist referral.
Biomarker-guided therapy — titrating medications to achieve a target NT-proBNP — was tested in the GUIDE-IT trial in HFrEF patients and did not improve outcomes compared to clinical management alone, although the target group received more medication intensification. Current ESC guidance recommends NT-proBNP for diagnosis and prognosis, not as a stand-alone titration target. The biomarker complements rather than replaces symptom assessment, weight monitoring, and physical examination.
In post-discharge heart failure care, an NT-proBNP that fails to fall by 30% within 30 days of an admission predicts a 2- to 3-fold increase in 90-day readmission risk. This subgroup warrants intensified follow-up, dose optimisation, and consideration of device therapy referral.
References
- PMID 7219045. PMID 7219045
- PMID: 25176015. PMID 25176015
- PMID 25282031. PMID 25282031
- Levin ER, Gardner DG, Samson WK. Natriuretic peptides. NEJM 1998;339:321–328. PMID 9682046
- PMID: 27206819. PMID 27206819
- PMID: 35379503. PMID 35379503
- PMID: 30025575. PMID 30025575
- PMID: 24076282. PMID 24076282