Hypothyroidism
Hypothyroidism is a state where the thyroid gland produces insufficient T3 and T4. Prevalence in women over 40 reaches 10%. Diagnosis: TSH above 4.0 mIU/L + symptoms (fatigue, weight gain, hair loss, cold intolerance).
hub
Evidence-based protocols for hypothyroidism, AIT, insulin resistance, and endocrine dysfunctions
The thyroid gland is the master metabolic regulator. This hub aggregates articles on clinical protocols for hypothyroidism, autoimmune thyroiditis, insulin resistance, adrenal dysfunction, and other endocrine disorders. Each article cites peer-reviewed sources (Lancet, NEJM, JAMA, Endocrine Reviews) with direct PubMed links.
Last reviewed: 2026-06-01 · Dr. V. Pereligyn
Hypothyroidism is a state where the thyroid gland produces insufficient T3 and T4. Prevalence in women over 40 reaches 10%. Diagnosis: TSH above 4.0 mIU/L + symptoms (fatigue, weight gain, hair loss, cold intolerance).
AIT is autoimmune destruction of thyrocytes with positive anti-TPO and/or anti-TG antibodies. The most common cause of hypothyroidism in iodine-sufficient regions. Often triggered by EBV reactivation, selenium deficiency, HPA-axis stress, post-partum.
Hyperthyroidism is excess thyroid hormone production. Graves is the autoimmune variant with TSH-receptor antibodies (TRAB). Symptoms: tachycardia, weight loss, tremor, exophthalmos. Differentiated from subacute thyroiditis and toxic adenoma.
Thyroid nodules are detected in up to 50% of people on screening ultrasound. Most are benign. Red flags: nodule growth, calcifications, hypoechogenicity, irregular borders — require TIRADS stratification and fine-needle aspiration if indicated.
Isolated TSH elevation (4.0-10.0 mIU/L) with normal fT3 and fT4. Most cases do not require therapy, but with positive anti-TPO, symptoms, pregnancy or preconception — NDT or L-T4 initiation is warranted.
| Marker | Reference | What it means |
|---|---|---|
| TSH (thyroid-stimulating hormone) | 0.4-4.0 mIU/L | Optimum 1.0-2.5. Primary screening marker. Elevated in hypo-, suppressed in hyperthyroidism. |
| Free T4 (fT4) | 11.5-22.7 pmol/L | Prohormone, peripherally converted to T3. Decreased in overt hypothyroidism. |
| Free T3 (fT3) | 3.5-6.5 pmol/L | Active hormone. fT3/fT4 ratio reflects peripheral conversion quality. |
| Anti-TPO (thyroid peroxidase antibodies) | <5.6 IU/mL | AIT marker. Positive → high risk of overt hypothyroidism within 5 years. |
| Anti-TG (thyroglobulin antibodies) | <4.1 IU/mL | Adjunct AIT marker + post-thyroidectomy monitoring in oncology. |
| TRAB (TSH-receptor antibodies) | <1.75 IU/L | Specific for Graves disease. Level correlates with severity. |
| Reverse T3 (rT3) | individual | Elevated in stress, infection, low-calorie diets. High rT3 blocks peripheral T3 action. |
NDT contains T3 and T4 in a ~1:4 ratio, close to physiological. In some patients with L-T4 intolerance (persistent fatigue, brain fog despite "normal" TSH), switching to NDT improves symptoms and peripheral hormone activity. Targets: TSH 0.5-2.0, fT3 in the upper third of the reference range. Recheck every 6-8 weeks during titration. [1][2][3]
LDN 1.5-4.5 mg at bedtime — off-label option for confirmed EBV reactivation or concurrent CFS/post-viral fatigue. Mechanism via TLR4 + TRPM3 restoration on NK cells. No direct AIT RCTs; justified in patients with systemic autoimmune-overlap patterns. [1][2][3]
Selenium 200 mcg/day as selenomethionine reduces anti-TPO by 20-40% over 3-6 months (RCT data). Effect persists only while supplementation continues. Simultaneous iodine is controversial — worsens AIT in a subset of patients. [1][2][3]
Ferritin <50 ng/mL and vitamin D <30 ng/mL impair T4→T3 conversion and normal immune response. Maintaining ferritin 70-100 and vitamin D 50-80 ng/mL is a mandatory part of the AIT protocol. [1][2][3]
A 38-year-old woman presented with fatigue, hair shedding, and 6 kg weight gain over one year. Baseline: TSH 4.8 mIU/L, free T4 11.2 pmol/L, free T3 3.9 pmol/L, anti-TPO 480 IU/mL, anti-Tg 92 IU/mL, ferritin 28 ng/mL. Diagnosis: autoimmune thyroiditis with subclinical hypothyroidism. Intervention: NDT 32.5 mg/day titrated to 65 mg/day over 6 weeks, selenomethionine 200 mcg/day, iron bisglycinate 50 mg/day. At 6-month review: TSH 1.4 mIU/L, free T3 5.1 pmol/L, anti-TPO 180 IU/mL (−63%), weight −4.2 kg, ferritin 78 ng/mL. Symptomatic recovery achieved.
A 45-year-old man, routine screening. Baseline: TSH 6.9 mIU/L (repeat at 8 weeks 7.2), free T4 13.4 pmol/L, anti-TPO 95 IU/mL, serum selenium 68 mcg/L, vitamin D 22 ng/mL. Diagnosis: subclinical hypothyroidism with autoimmune features. Levothyroxine deferred given TSH <10. Intervention: selenomethionine 200 mcg/day, low-dose naltrexone 3 mg nightly, cholecalciferol 4000 IU/day. At 4-month review: TSH 2.6 mIU/L, anti-TPO 41 IU/mL (−57%), selenium 118 mcg/L, vitamin D 48 ng/mL. Euthyroid status reached without thyroid hormone replacement.
Lab reference for TSH is 0.4-4.0 mIU/L, but symptomatic optimum is 1.0-2.5. In AIT patients the target is 0.5-2.0. TSH above 2.5 with symptoms (fatigue, weight gain, hair loss) warrants evaluation of anti-TPO, fT3, fT4, and discussion of therapy initiation.
Levothyroxine contains only T4 (relying on effective peripheral conversion to T3). NDT (Thyroid-S, Armour) is natural porcine thyroid extract with T3 and T4 in ~1:4 ratio. With impaired conversion or persistent symptoms despite "normal" TSH, NDT is often better tolerated.
Iodine in AIT is controversial. In some patients, high-dose iodine intensifies the autoimmune process and raises anti-TPO. With AIT, iodine is reasonable only with proven deficiency (urinary iodine <100 mcg/L) and at physiologic doses 100-150 mcg/day.
Full AIT regression without relapse is rare. A realistic goal is 50-80% anti-TPO reduction, normalized TSH, and symptom resolution. This is achieved by combining adequate replacement (NDT/L-T4), selenium, ferritin and vitamin D maintenance, and trigger elimination (stress, EBV, sleep deficit).
First TSH + fT3 + fT4 recheck — 6-8 weeks after initiation or dose adjustment. Earlier — hormones have not reached a new steady-state. After stabilization — every 3-6 months. In pregnancy — every 4 weeks in the first trimester.
Directly — no. But chronic stress via the HPA-axis raises rT3, impairs T4→T3 conversion, and activates autoimmune processes. In genetically susceptible patients, prolonged stress is often the trigger for AIT manifestation.

A patient has been on antidepressants for five years with no lasting effect — nobody ever checked TPO antibodies. A case-control study found the lifetime odds of depression are 6.6× higher, and generalized anxiety disorder 4.9× higher, in patients with euthyroid Hashimoto's — with completely normal TSH and fT4. I review exactly which mental illnesses are linked to thyroid disease, the mechanism, and when adding T3 works as an antidepressant strategy.

When a clinician orders "just TSH" — they measure pituitary function, not thyroid function. TSH is a late, inertial marker: it reflects chronic imbalance, not acute dysfunction. Estrogens, biotin, non-thyroidal illness, circadian rhythm — all shift the number without changing thyroid status. Here is the full panel and the decision principle.

T3 is the only thyroid hormone that actually works. And it works not in blood but inside the cell, at the nuclear receptor. Blood is only a transport phase. Some women with normal TSH have cellular hypothyroidism and suffer with full symptoms despite "normal" labs. Here is the biology of T3, T4→T3 conversion, the hidden forms of deficiency, and the full laboratory panel.

The patient has been on levothyroxine for five years, TSH is normal — yet hypothyroid symptoms persist. This is not "poor compliance"; it is a systems failure: peripheral T4→T3 conversion, membrane transport, cofactors, cortisol, gut. We break down what general practice misses and what protocol actually works — with PMIDs, doses, and 8-week control markers.

TSH normal, free T4 normal, and the patient is falling apart with fatigue, cold intolerance, weight gain, and broken sleep. The classic "your labs are fine" trap. In reality, chronic stress shuts the thyroid down at three different levels, and you only see it on a properly built panel: fT3, rT3, salivary cortisol, ferritin, selenium. Here is the mechanism, the exact numbers, and an 8-week recovery protocol.

Two to six weeks after an acute viral infection, the patient returns with "I am not myself" complaints: palpitations, sweating, anxiety — or the opposite, fatigue, edema, apathy. The post-viral thyroid can follow one of three clinically distinct paths. Treatment for each is different. Blanket therapy makes things worse. This review covers how to tell the scenarios apart, what to measure, and when not to prescribe levothyroxine.

Anti-TPO antibodies are the key to diagnosing autoimmune thyroiditis — but not a treatment target and not a reason for repeat testing. Here is when the test changes management, how to read the titer (35 / 100 / 1000 IU/mL), why an isolated positive without ultrasound and clinical signs is a lab finding rather than Hashimoto, and where selenium actually reduces antibody levels by 30–40%.

Hashimoto's thyroiditis is not a snapshot diagnosis — it is a slow autoimmune process that unfolds over 10–30 years through four sequential stages. Understanding the stage changes clinical strategy: starting levothyroxine in stage 1 is blind therapy; withholding it in stage 3 is malpractice. This article maps the four stages with markers, timing, and the protocol grounded in ATA Guideline.

Up to 50% of adults have thyroid nodules on ultrasound. The vast majority are benign. The decision to biopsy is not made on the fact of detection but on the TIRADS category combined with size. This review covers the practical ACR TIRADS scale, size thresholds for biopsy, the surveillance protocol, and where Bethesda fits after FNA.

Selenium is the obligate cofactor of deiodinases and glutathione peroxidases, and the thyroid gland concentrates it more densely than any other organ per gram of tissue. In Hashimoto's thyroiditis, 200 mcg for 6 months reduces TPO antibodies by 30–40%. Less is sub-optimal, more is selenosis. This is the analysis: why exactly this dose, which form works, when selenium is useless, and how to monitor therapy.

What is "normal" for a non-pregnant woman can be hypothyroidism for the fetus. Until weeks 18–20, the fetal CNS develops entirely on maternal thyroid hormones. Here are trimester-specific TSH targets, tactics for anti-TPO positive women, levothyroxine dosing, and iodine prophylaxis per ATA 2017 (PMID 28056690).

Vitamin D raises calcium absorption but does not decide where that calcium goes. Vitamin K2 (menaquinone MK-7) does: into bone via osteocalcin activation, or into arterial walls when deficient. In Hashimoto autoimmune thyroiditis this pair is critical — hypothyroidism itself increases the risk of osteoporosis and vascular calcification. Exact doses, 25(OH)D targets, monitoring, contraindications, and the protocol with levothyroxine.

After thyroid removal, 10–15% of patients on adequate L-thyroxine and "normal" TSH continue to report fatigue, weight gain, cognitive issues. This is not "all in your head" — it is incomplete T4-to-T3 conversion. I break down the US protocol for NDT: composition, brands (Armour, NP Thyroid, ADTHYZA), starting doses, titration, and when L-thyroxine remains the correct choice.

TSH is "in range" and the patient still has no energy. Up to one in three patients on adequate levothyroxine continues to report residual symptoms. Fatigue runs along three independent axes — T4→T3 conversion, cofactor status (Fe, D3, Mg), and HPA cortisol. Thyroxine closes only one of them. This review covers what to measure beyond TSH and how to start targeted correction based on the result.

Naltrexone at 1.5–4.5 mg/day (10 times lower than addiction-medicine dosing) ceases to act primarily as an antagonist and becomes an immunomodulator. Short nocturnal blockade of μ-opioid receptors produces a rebound increase in endogenous endorphins, TLR4 blockade on microglia, and a Th17 / Treg shift toward tolerance. In Hashimoto thyroiditis, LDN is a third-line candidate when TPO antibodies remain elevated despite an adequate L-T4 dose and corrected selenium and vitamin D deficiencies. I review the mechanism, titration protocol, expected time to effect, and settings where LDN should not be used.
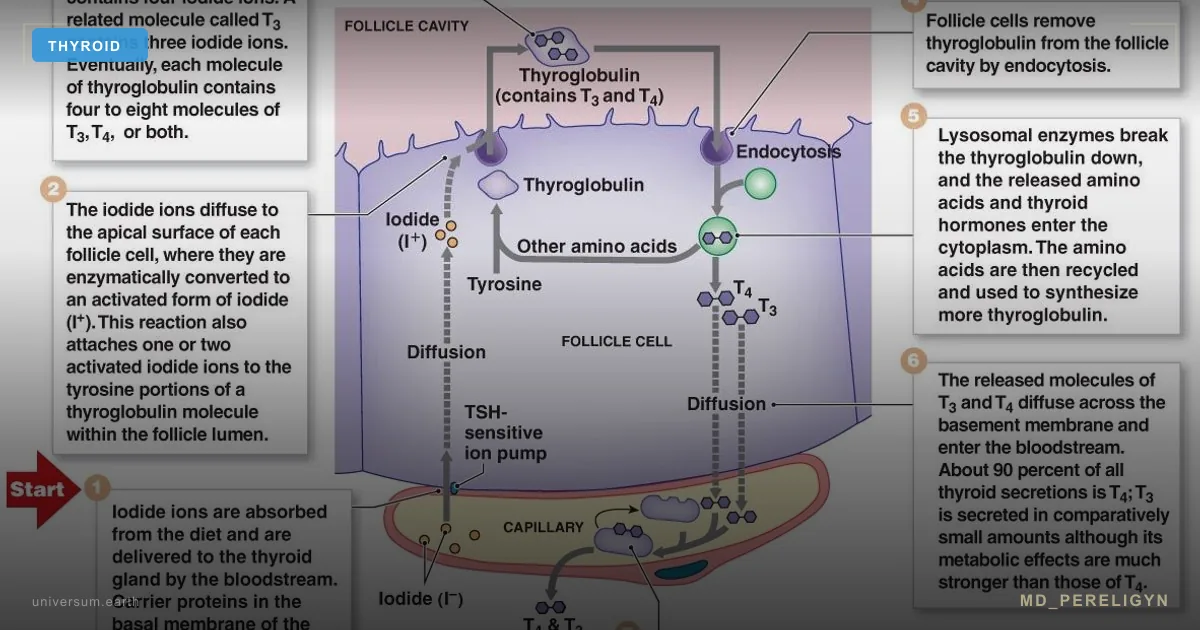
Thyroxine (T4) is a prohormone; the active hormonal form is triiodothyronine (T3). The D1/D2 deiodinase enzyme in the liver, kidneys, intestine, and brain is responsible for T4 → T3 conversion. If the enzyme is not properly assembled from selenium, iron, and zinc, the tablet remains in the bloodstream while tissues remain without a signal. Every third patient on an L-thyroxine dose that is adequate by TSH continues to feel unwell: fatigue, dry skin, hair loss, weight gain, brain fog. This is functional hypothyroidism: a state in which TSH is normal, fT4 is normal, but tissue T3 is not. I review four mechanisms of impaired conversion, markers, target ranges, and a holistic restoration protocol.

When labs show elevated prolactin, women are often sent for pituitary MRI under the assumption of a prolactinoma. But in the vast majority of cases, this is not about a tumor — it is about dysregulation of dopaminergic control. Understanding this changes both diagnostics and treatment approach.

L-thyroxine + OCPs to a young woman "just in case" — this is not treatment, it is intervention into the endocrine axis without diagnosis. Let us examine how ethinyl estradiol distorts thyroid labs and why the standard "elevated TSH → give thyroxine" approach often contradicts current clinical guidelines.

Iodine is essential raw material for thyroid hormones, but 80% of cases of its inefficacy or harm are not about dose — they are about systemic context. When selenium and iron are missing, iodine does not heal — it fuels inflammation. Here is the five-stage model: from cellular uptake to T4→T3 conversion.

When you aggressively cut calories, fast, and live in stress, the body does not turn on fat burning — it turns on survival mode. First water leaves and it seems to work. Then reverse T3 rises, active T3 falls, mitochondria slow, you feel cold, swollen, foggy. And weight stalls or creeps up. Here is how to escape this trap.
The term "adrenal fatigue" dominates integrative medicine discussions, yet it has never been recognized as a legitimate medical diagnosis. The real issue — HPA axis dysregulation — is well-documented in peer-reviewed literature and has measurable biomarkers, distinct phases, and evidence-based treatment protocols.
After age 40, testosterone declines by 1-2% annually. But age-related decline is not always benign. We examine when TRT is genuinely warranted, which labs are essential, and how to optimize testosterone naturally before committing to lifelong therapy.
Menopause affects every woman. But hot flashes, insomnia, anxiety, and bone loss are not inevitable. We examine the difference between bioidentical and synthetic hormone therapy, reinterpret the WHI study, and outline a personalized approach to menopausal hormone therapy.
In 70% of women with PCOS, the root cause is insulin resistance, not a hormonal imbalance. Standard birth control prescriptions mask symptoms without addressing the underlying mechanism. We examine the pathophysiology, proper diagnosis, and a comprehensive treatment protocol.

Pregnenolone — the precursor to every steroid hormone in the body — occupies a unique position at the intersection of endocrinology and neuroscience. During chronic stress and burnout, its levels decline among the first, triggering a cascade of hormonal disruption.
Labs are normal but symptoms persist? 15-20% of patients on levothyroxine continue to suffer from fatigue, weight gain, and brain fog. The problem isn't the patient — it's the approach.
Dr. Pereligyn offers in-person and online consultations.
Book a consultation